Created by Jiří Kofránek
Struktura přednášky
https://www.wikilectures.eu/w/Respiratory_insufficiency
https://www.wikilectures.eu/w/Cardiopulmonary_monitoring
>=50 g O2/l reduced Hb
150 g/l <75%
in anemia will not
50 g/l - anemia, pale
polycythemia vera >165 g/l men 160 women
JAK2 mutation clonal mutation (cyanosis)
g/l *0.06205784→ mmol/l
mmol/l*16.114→ g/l
differentiated from peripheral - tongue
but be careful . peripheral can be masked by hypoperfusion (fingers are pale)
https://www.wikilectures.eu/w/Glasgow_Coma_Scale
GCS, 15-13 OK, 12 -9 moderate, 8-3 impaired consciousness
GCS 15 ok
Respiratory rate above 22 - saturation OK,
Respiratory rate 30 - attention
90% - PO2 60 mmHg
Respiratory rate above 22 - saturation OK,
Respiratory rate 30 - caution
https://egolem.online/bloodgases/#pribeh2a.md
PaO2/FiO2 norm 100 mmHg/0.21 = approximately 500 (300-500 is the norm)
P-F ratio PaO2 300-500 is the norm
300 - 200 mild damage
200-100 moderate damage
100 and less - severe damage (ARDS)
https://en.wikipedia.org/wiki/Horowitz_index
PaO2 <60 mmHg
(60 mmHg corresponds to approximately 90% saturation)
PCO2 > 50 mmHg
pH <7.3 -> consider artificial ventilation
Low PaO2
PaCO2 normal or low (respiratory alkalosis)
Within a week
Months, years
in seniors
antibodies against nicotinic receptors (to acetylcholine) ← Ig (worsens during the day)
diffuse edema (ground glass X-ray)
wedge pressure <18 / cardiac cause ruled out
![]() Acute respiratory distress syndrom v3.pptx
Acute respiratory distress syndrom v3.pptx
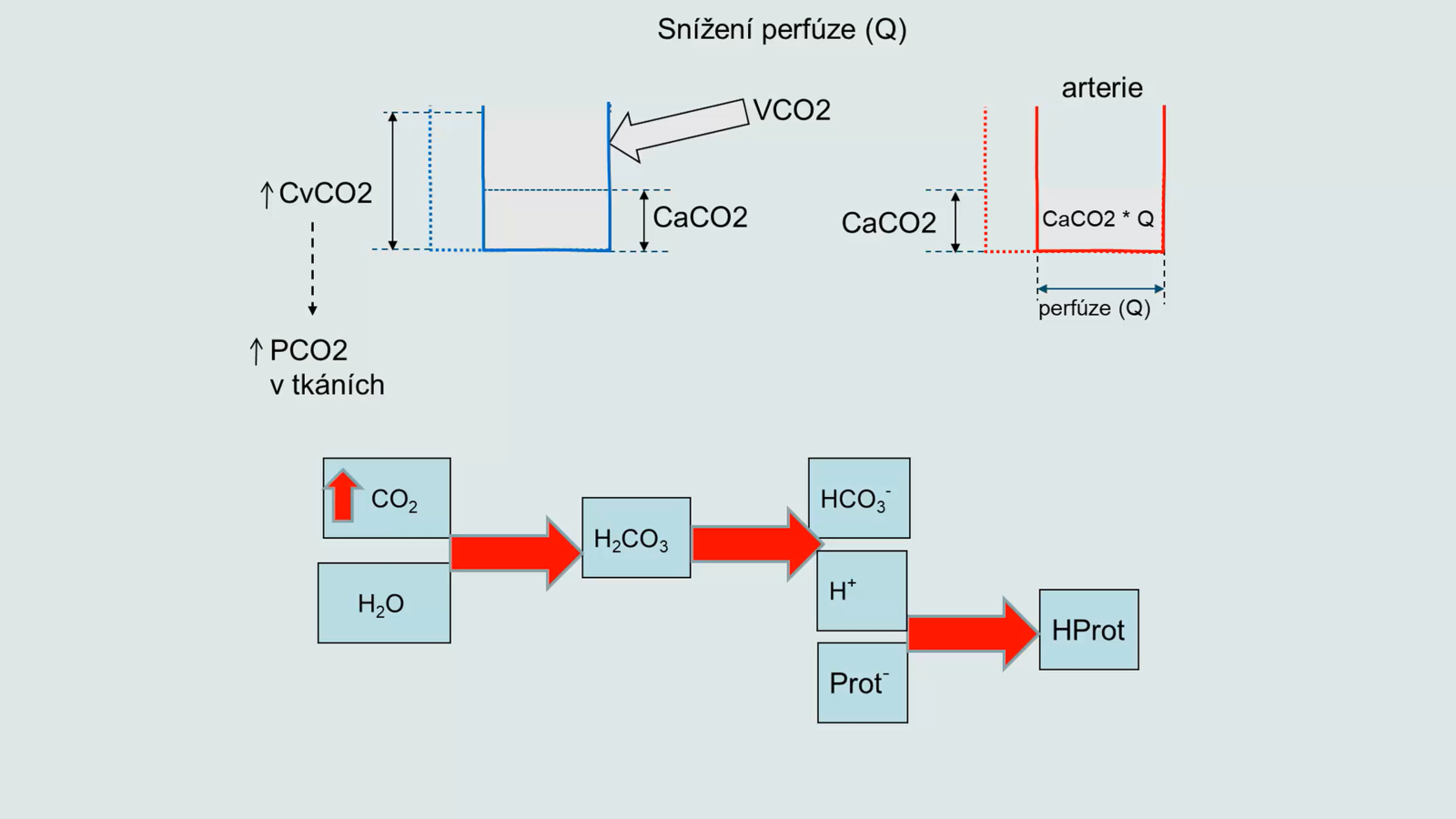
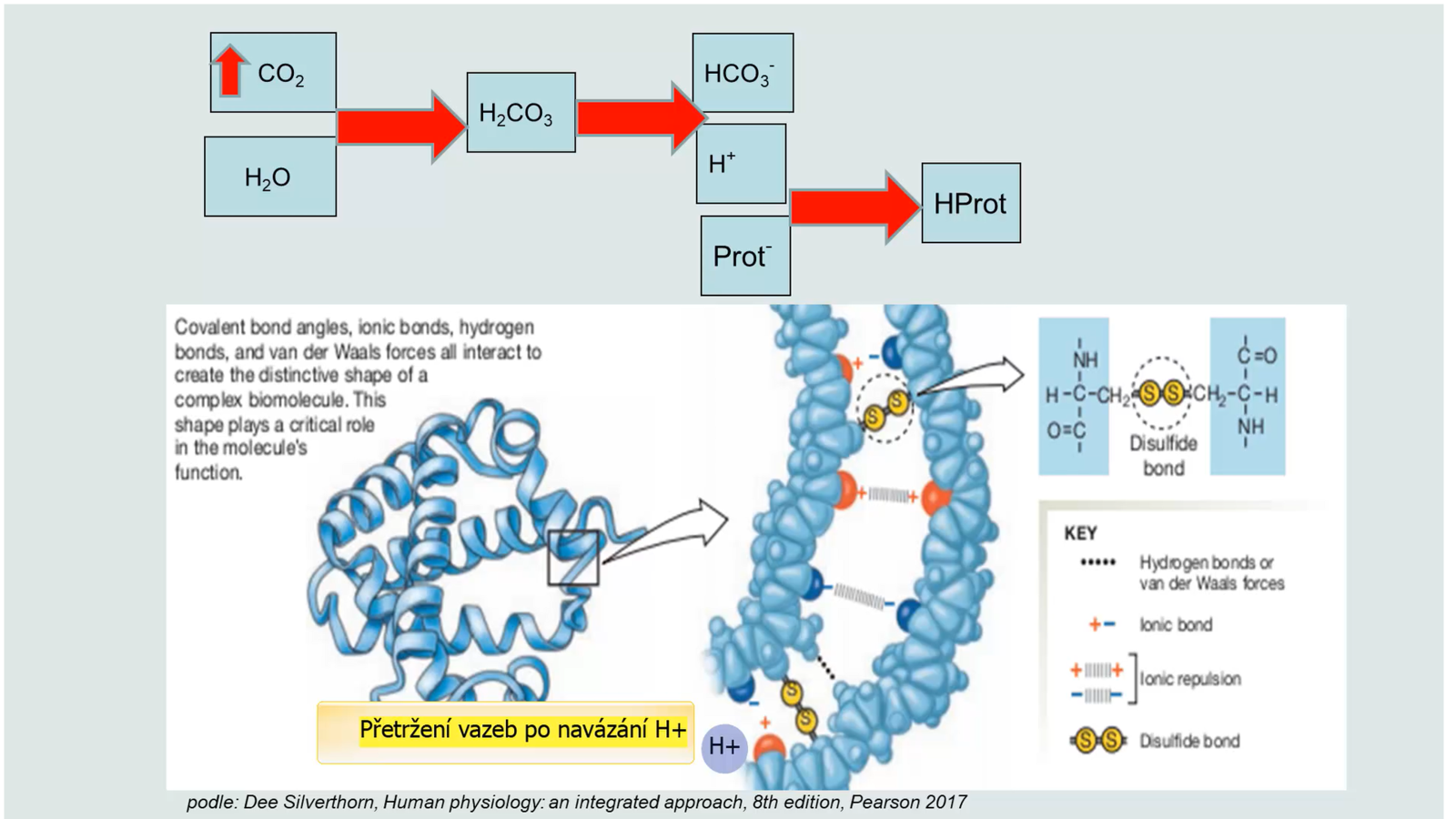
bicarbonate
protein
hemoglobin
phosphate (IC)
... while the alveoli do not hyperventilate - alveolar ventilation does not change
The goal is cooling - thermoregulation
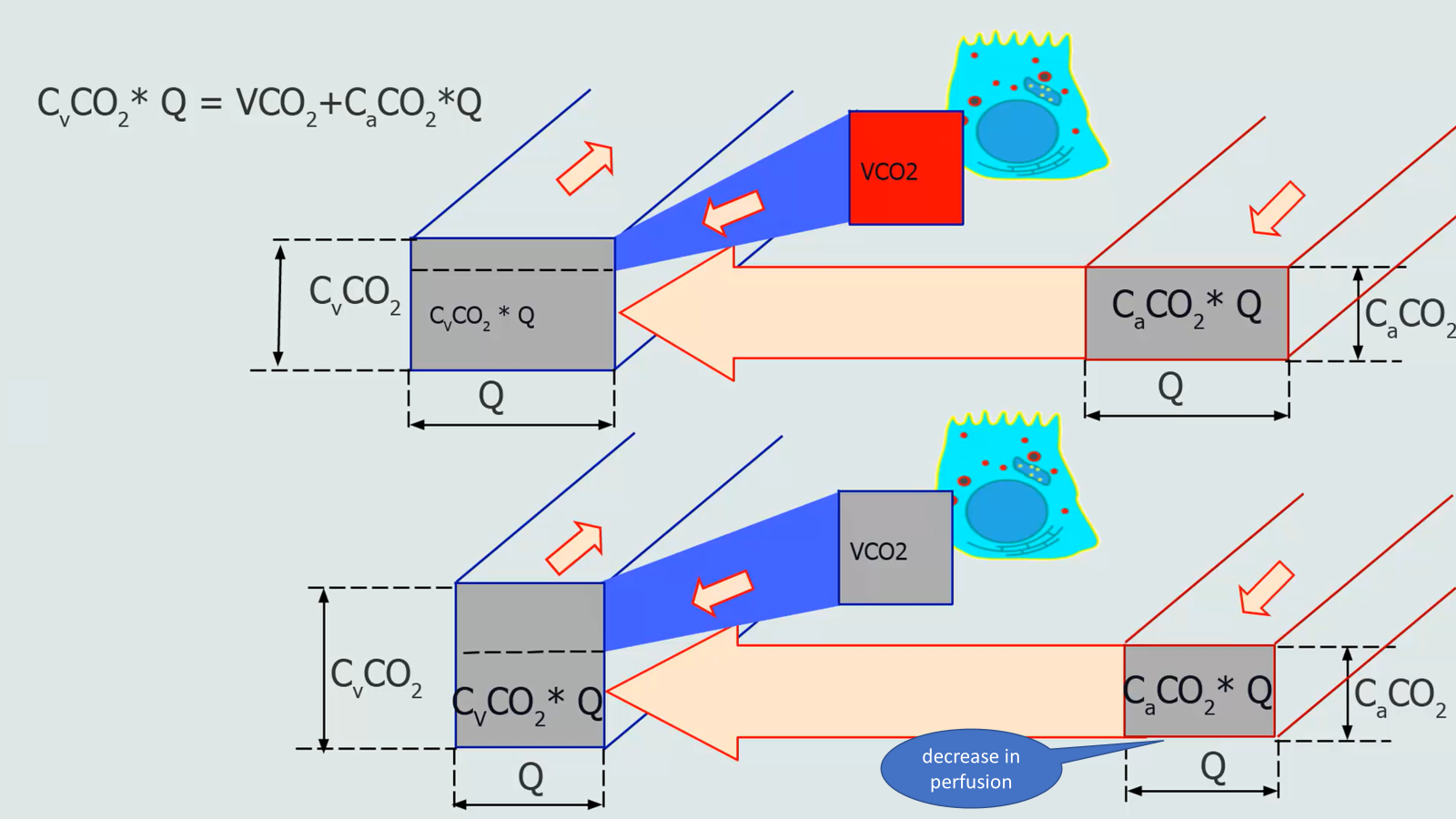
there is no ventilation and there is perfusion