Respiratory insufficiency
Created by Jiří Kofránek

Respiratory insufficiency (failure)
Symptoms
Cardiopulmonary monitoring
https://www.wikiskripta.eu/w/Kardiopulmon%C3%A1ln%C3%AD_monitoring
Stuffiness Shortness of breath (dyspnoea)
But shortness of breath is also present in anemia
Shortness of breath is also present in cardiac failure - mainly of the left heart (pulmonary edema)
Tachypnea
involvement of auxiliary respiratory muscles
Cyanosis
>=50 g O2/l reduced Hb
150 g/l <75%
it will not be for anemia
50 g/l - anemia, pale
polycythemia vera >165 g/l men 160 women
JAK2 mutation clonal mutation (cyanosis)
g/l *0.06205784→ mmol/l
mmol/l*16.114→ g/l
https://egolem.online/bloodgases/#pribeh2a.md
central
differentiation from peripheral: tongue
but be careful. peripheral may be masked by hypoperfusion (fingers are pale)
peripheral
disorders of consciousness - disorientation - up to delirium
https://www.wikiskripta.eu/w/Glasgow_Coma_Scale
GCS, 15-13 OK, 12 -9 moderate, 8-3 impaired consciousness
GCS 15 ok
Respiratory rate
Respiratory frequency above 22 - saturation OK,
Respiratory rate 30 - attention
Laboratory measurement
O2 saturation
90% - PO2 60 mmHg
Respiratory frequency above 22 - saturation OK,
Respiratory rate 30 - attention
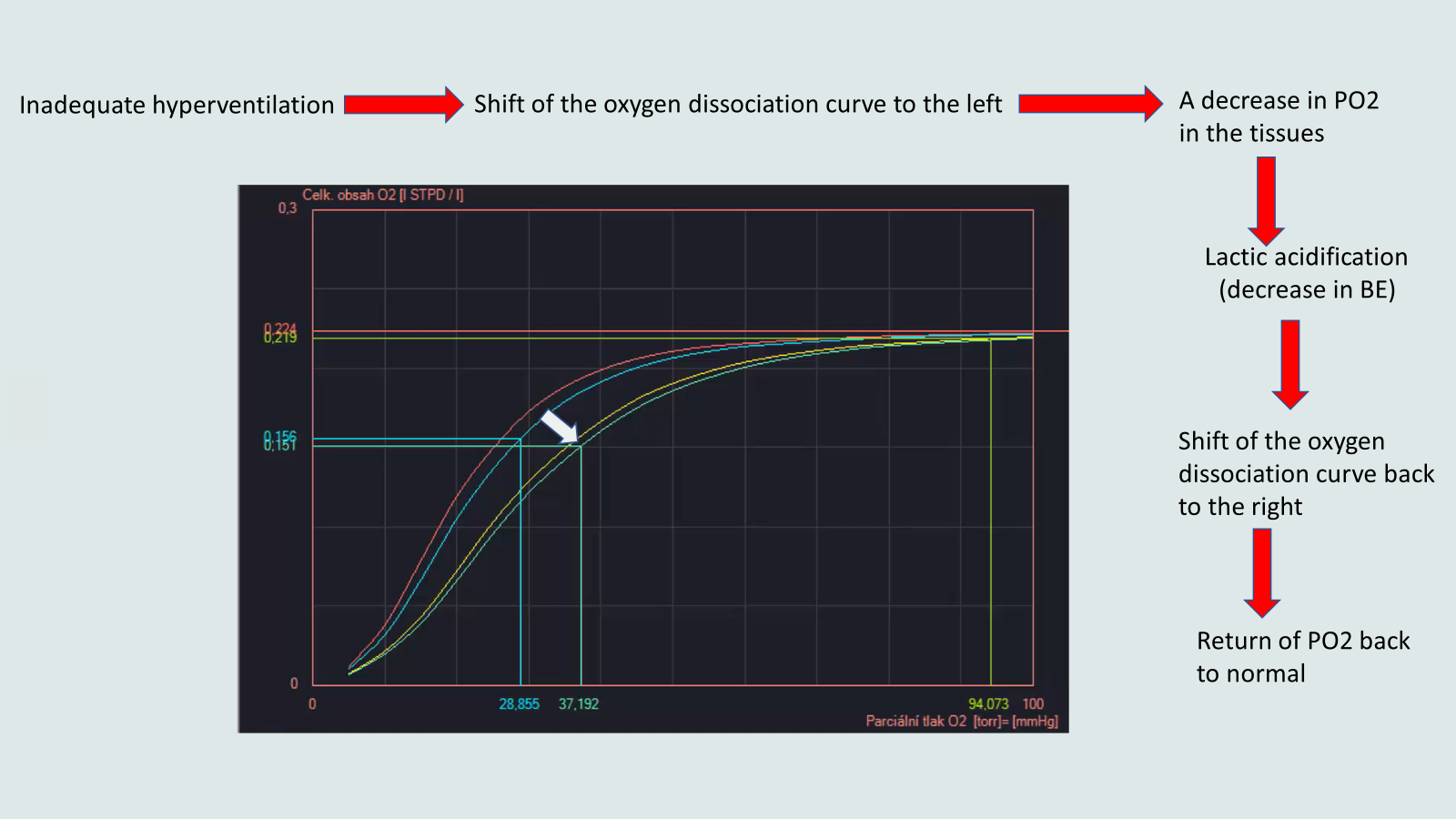
O2 and CO2 saturation curves
https://egolem.online/bloodgases/#pribeh2a.md
Masks the reduction in saturation
Oxygen supplementation
Heart rate
Horowitz Index (1970)
PaO2/FiO2 norm 100 mmHg/0.21 = approximately 500 (300-500 is the norm)
P-F ratio PaO2 300-500 is the norm
300 - 200 light damage
200-100 medium damage
100 and below - severe injury (ARDS)
https://en.wikipedia.org/wiki/Horowitz_index
Measurement of acid-base balance (Astrup) - PO2, PCO2, pH
PaO2 <60 mmHg
(60 mmHg corresponds to approx. 90% saturation)
PCO2 > 50 mmHg
pH <7.3 -> consider artificial ventilation
According to arterial PaO2, PaCO2
Type 1 partial (hypoxic)
Low PaO2
PaCO2 normal or low (respiratory alkalosis)
PaO2 <60 mmHg
PaCO2 norm or low → Respiratory alkalosis
From the onset of lung disease (before the respiratory muscles tire)
Type 2 global (hypoxic-hypercapnic)
PaCO2 >50 mm Hg -> respiratory acidosis
PaO2<60 mmHg
PaCO2 >50mmHg
According to time
Acute
Within a week
Acute onset - aspiration, ARDS (3 days)
Chronic
Months, years
It can become acute
COPD, Astma
Restrictive lung disorders
Causes of respiratory failure
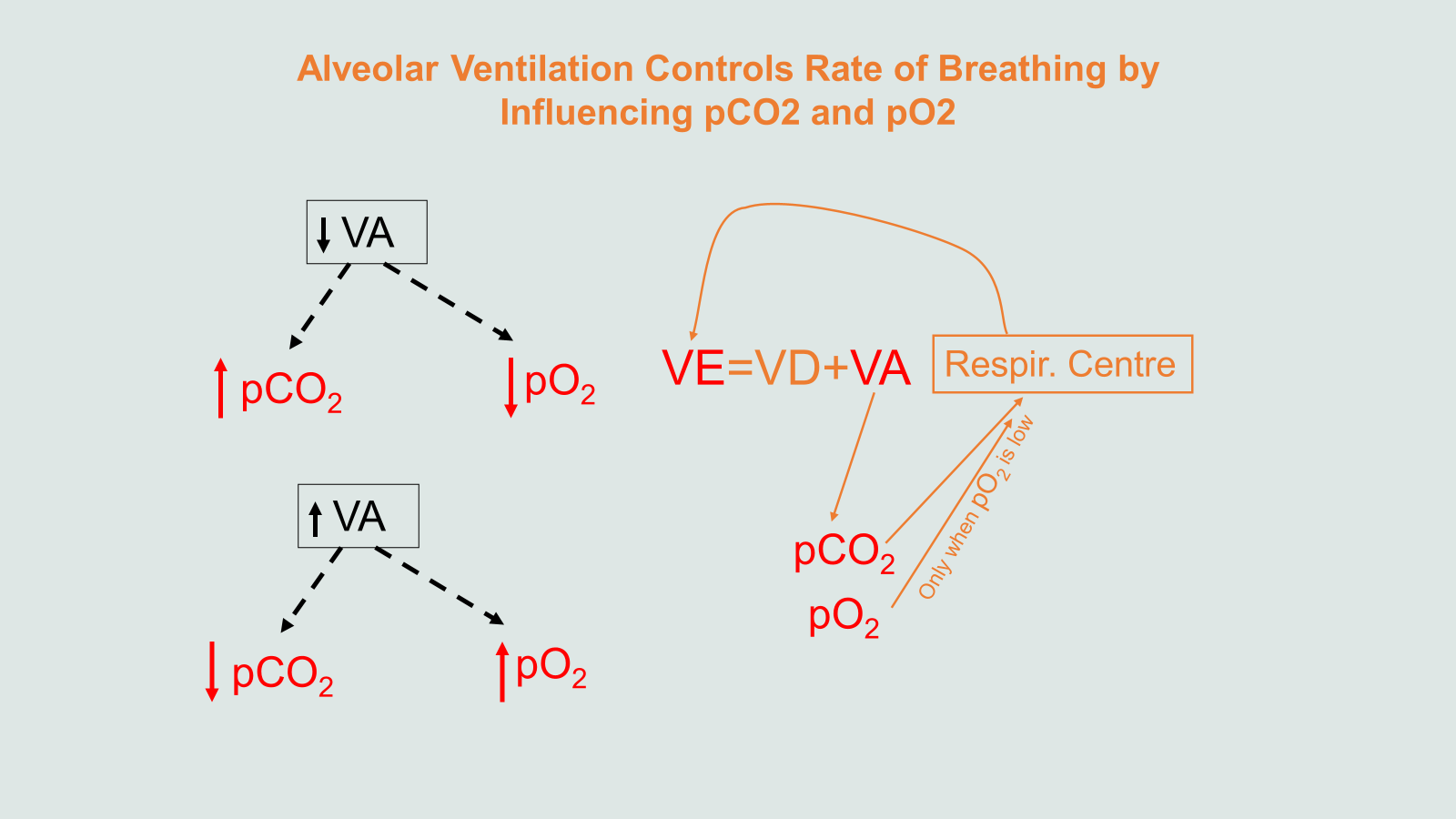
hypoventilation
Obstruction
Diffusion
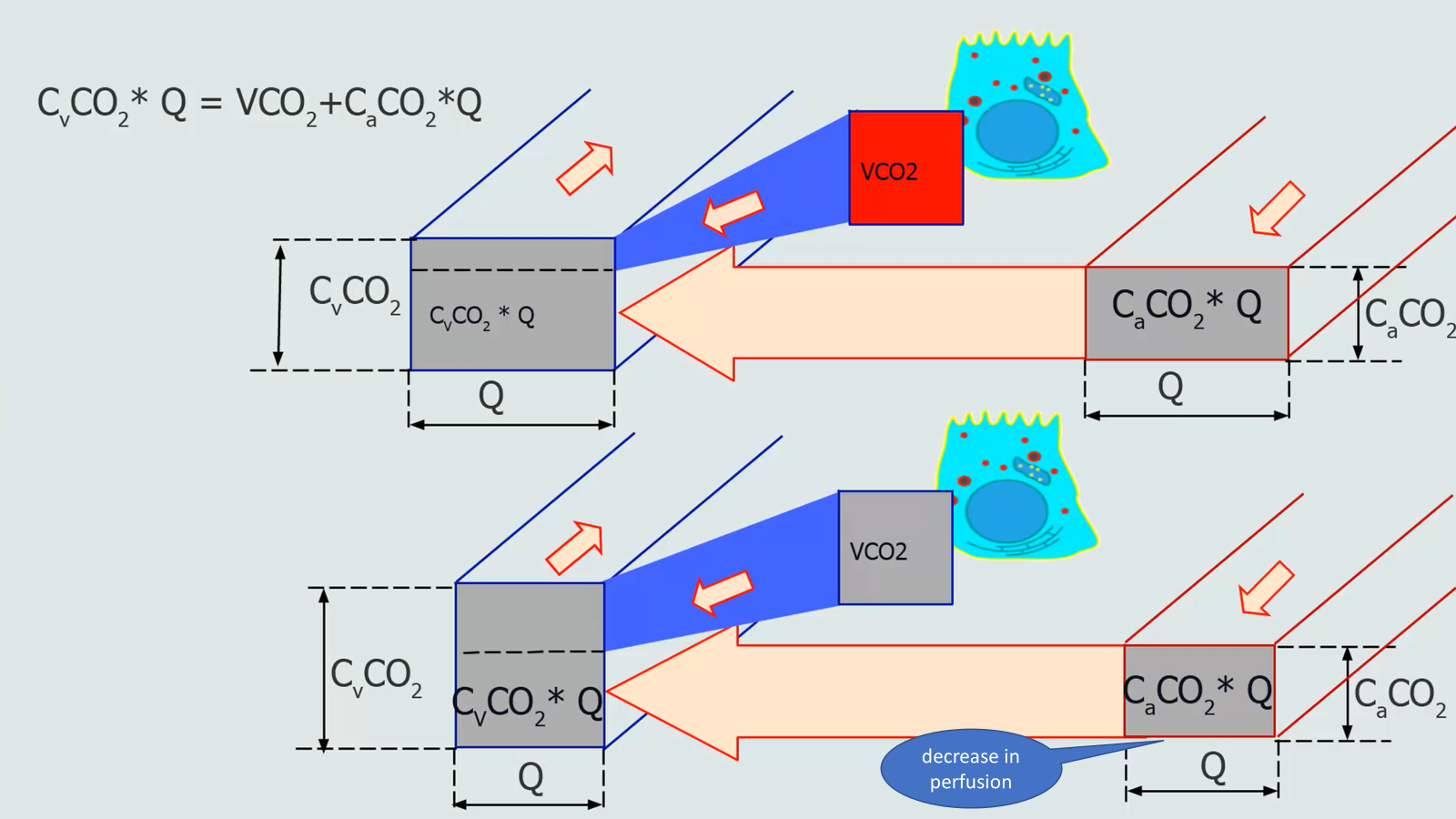
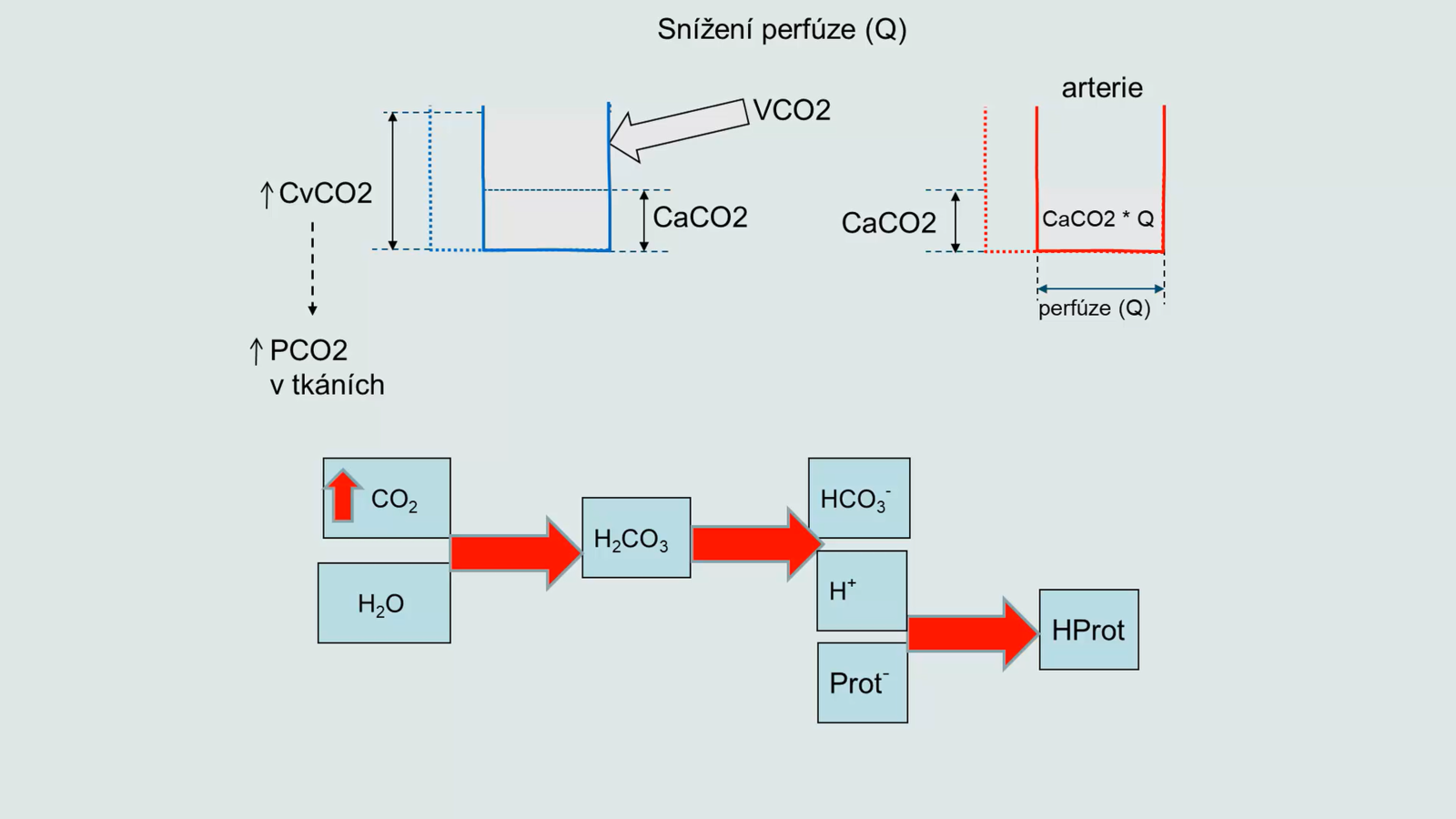
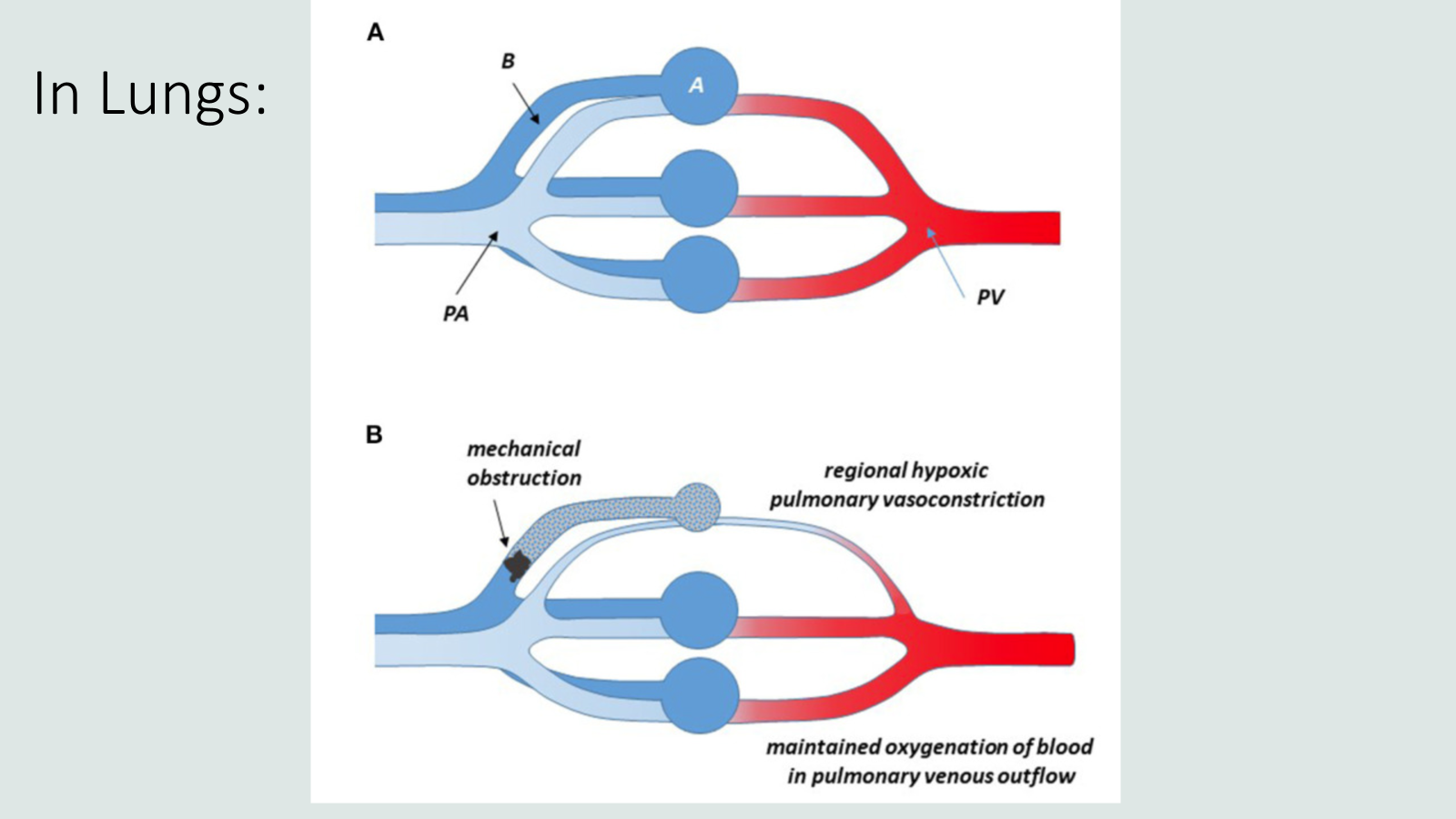
Perfusion → ventilation-perfusion V/Q ratio
Kyphoscoliosis
u seniorů
Obesity
Muscular dystrophy (Duchenne muscular dystrophy, Amyotrophic lateral sclerosis)
Myasthenia gravis
antibodies against nicotinic receptors (to acetylcholine) ← Ig (worsening during the day)
aphragmatic fatigue (after tachypnea)
CNS trauma, stroke
Spinal cord injury C3-C5 (phrenicus)
Opiates
PaC02 will increase - respiratory acidosis
Foreign body in the respiratory tract
Tumor, enlarged lymph nodes
Athma, COPD
VA/Q
Pneumonia
Cardiogenic edema
Noncardiogenic edema
ARDS
difúzní edém (RTG obraz mléčného skla)
tlak v zaklínění <18 /vyločení kardiální příčiny
Sepsis, gastric juice inspiration, hot air...
Acute respiratory distress
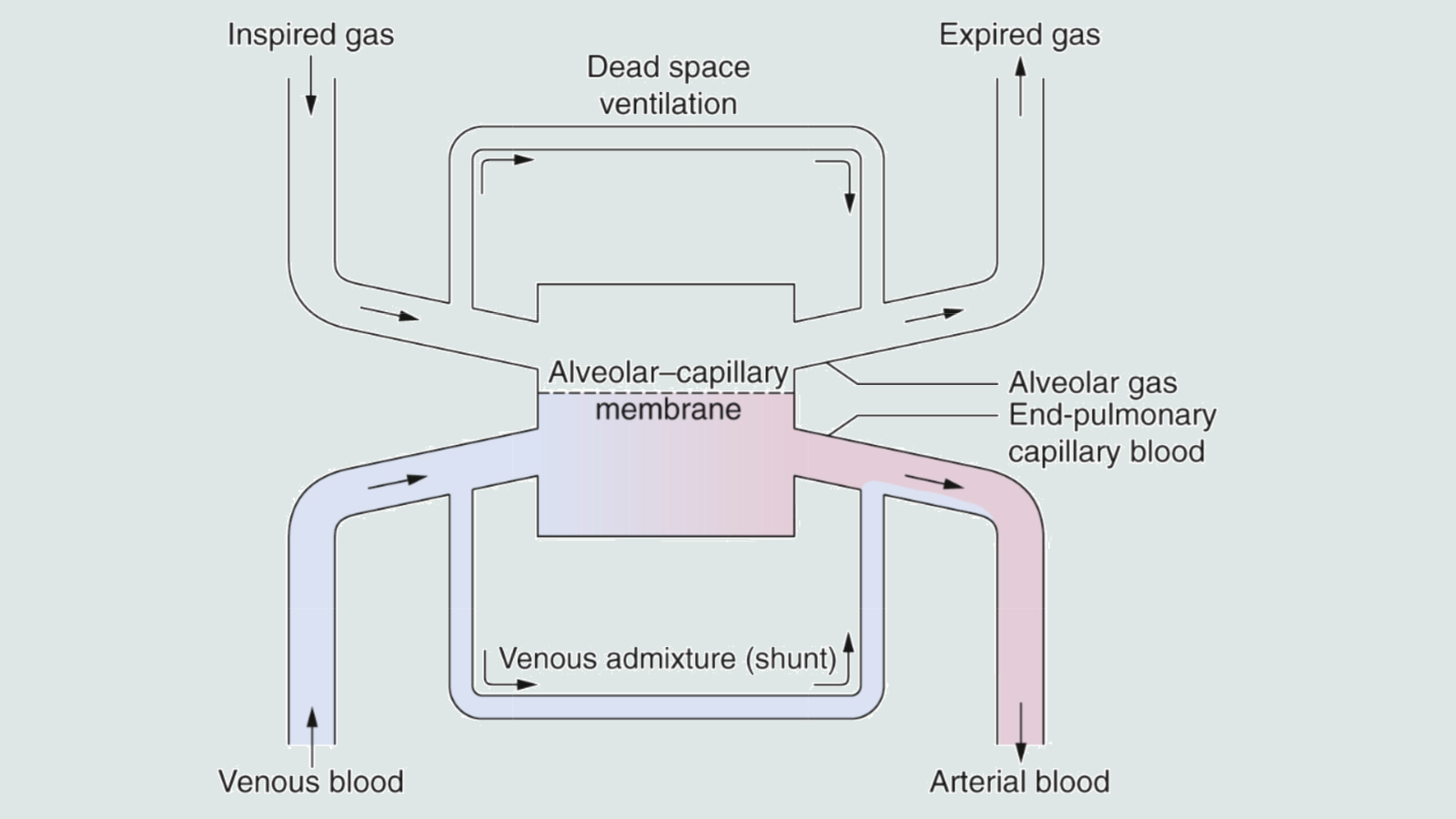
Ventilation without perfusion: dead space
Right-to-left shunts (RL shunts)
there is no ventilation but there is perfusion
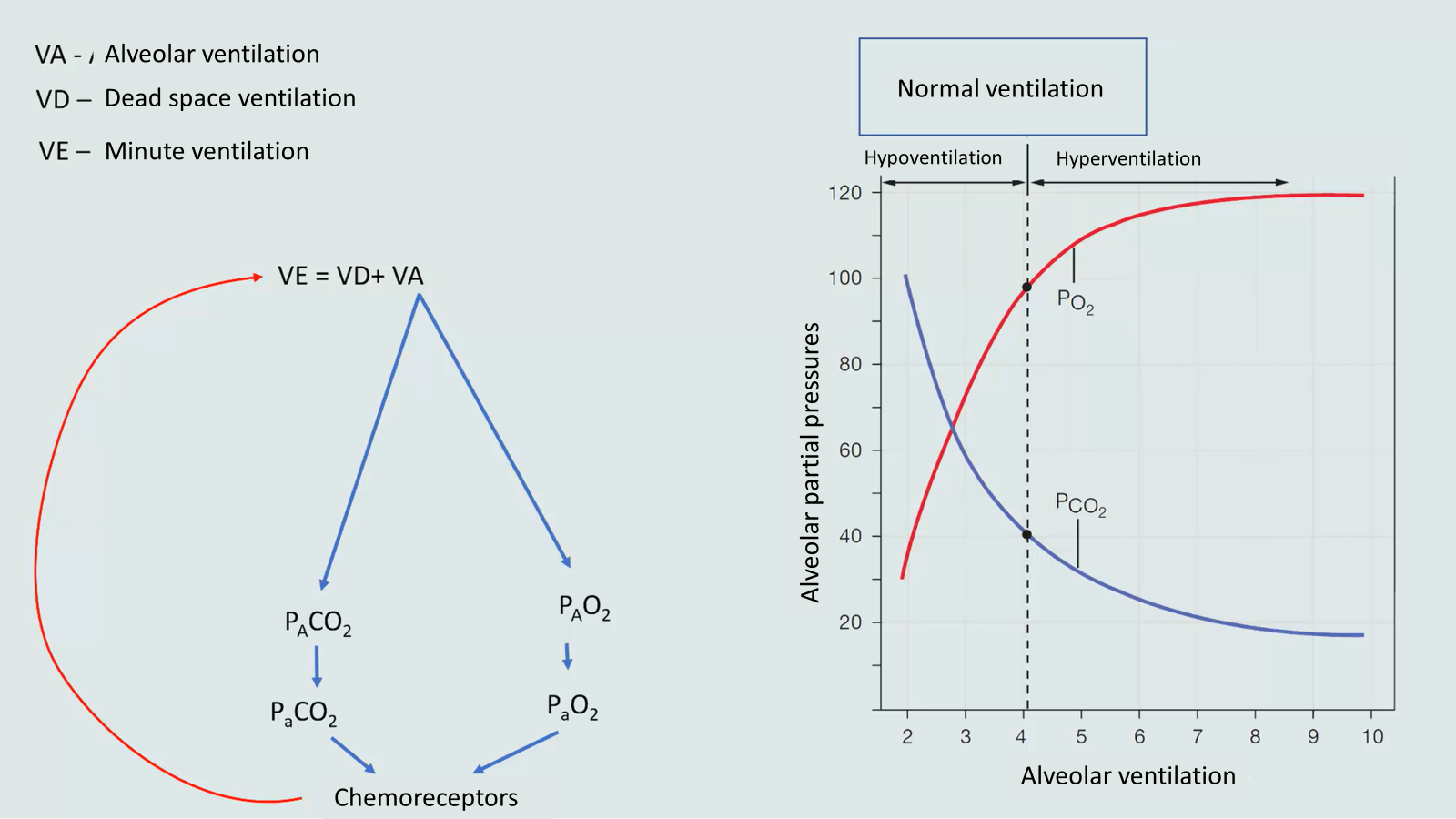
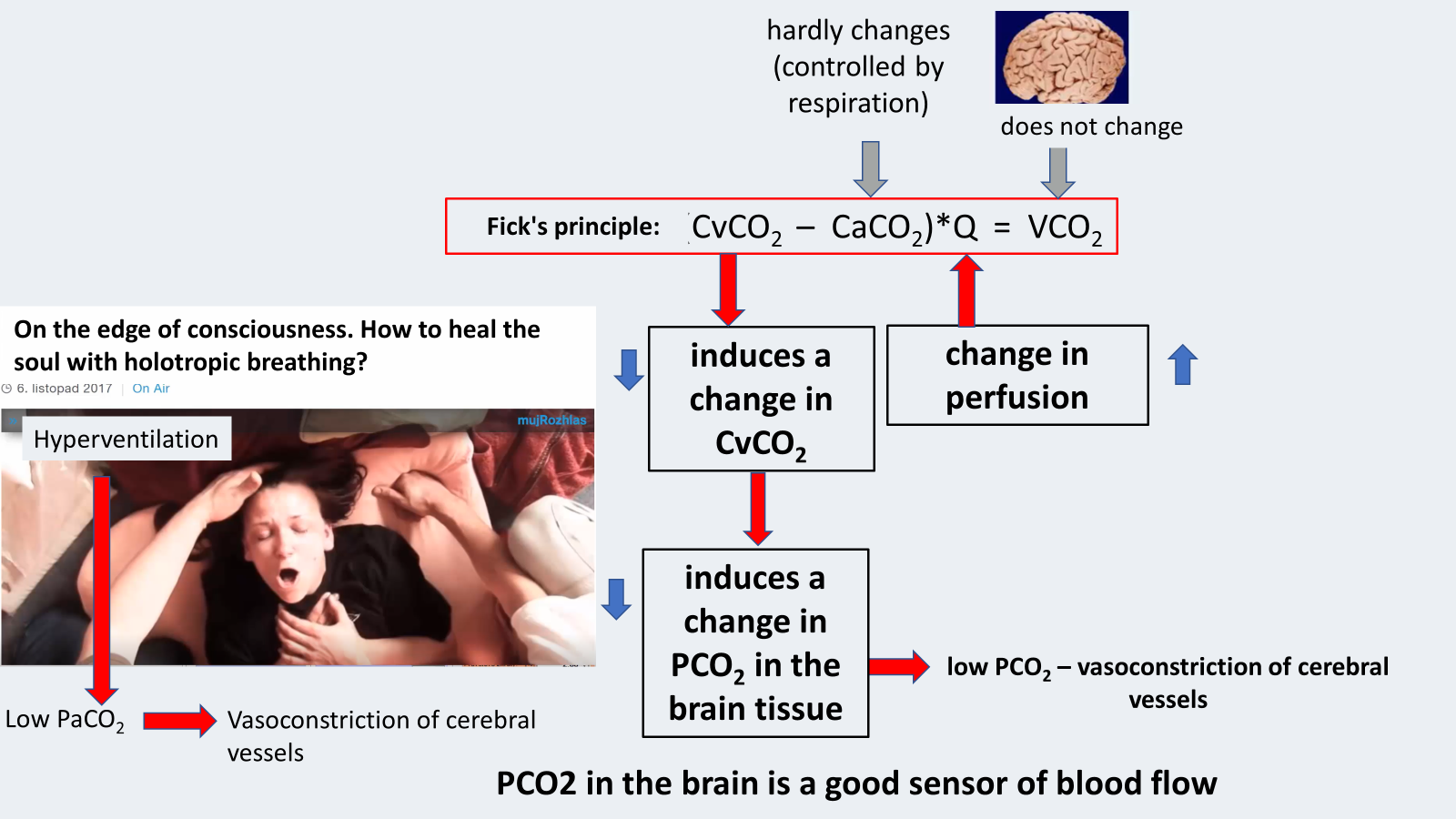
Hyperventilation
PaO2 will decrease
Breathing pattern of low -CO2 - hypocapnia
Tongue-out dogs hyperventilate the dead space, not the alveoli
... at the same time they do not hyperventilate the alveoli - alveolar ventilation does not change
The goal is cooling - thermoregulation
Hyperventilation
Kussmaul respiration
kusmaulovo dýcháníKussmaul respiration
PaO2 will only increase slightly
PaCO2 will decrease
Compensation of metabolic acidosis
Buffers
bicarbonate
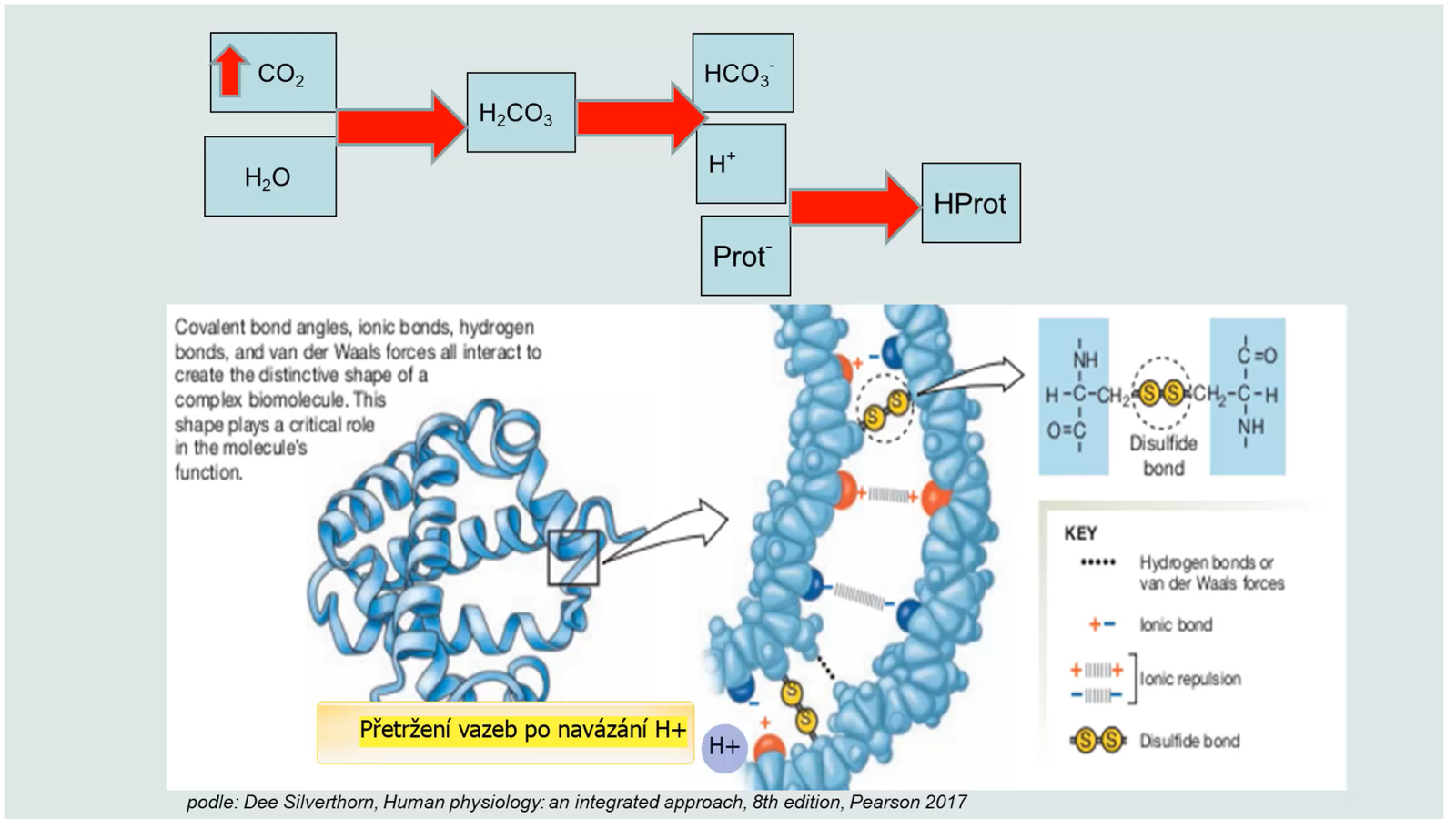
proteins
hemoglobin
phosphate (IC)
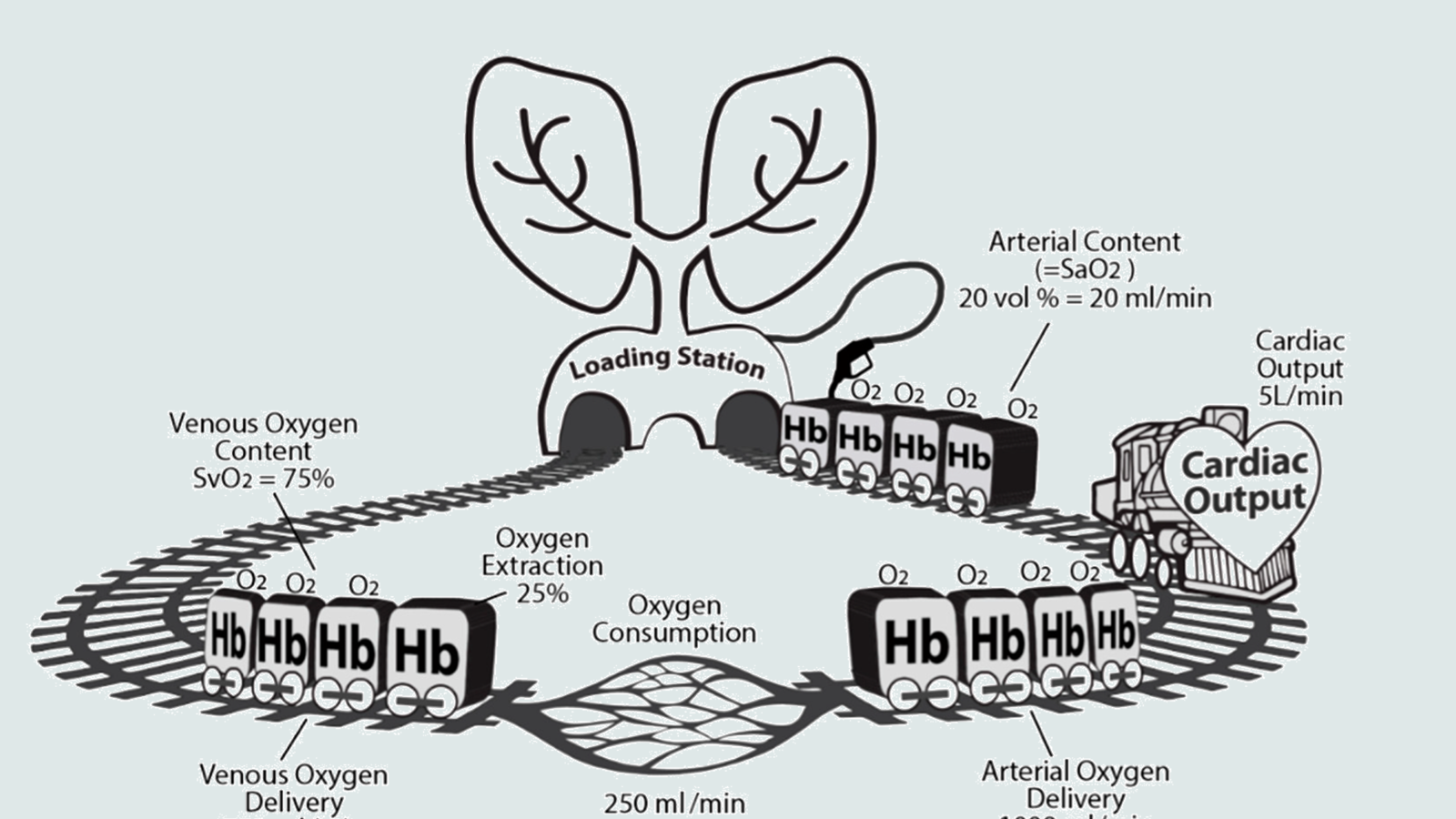
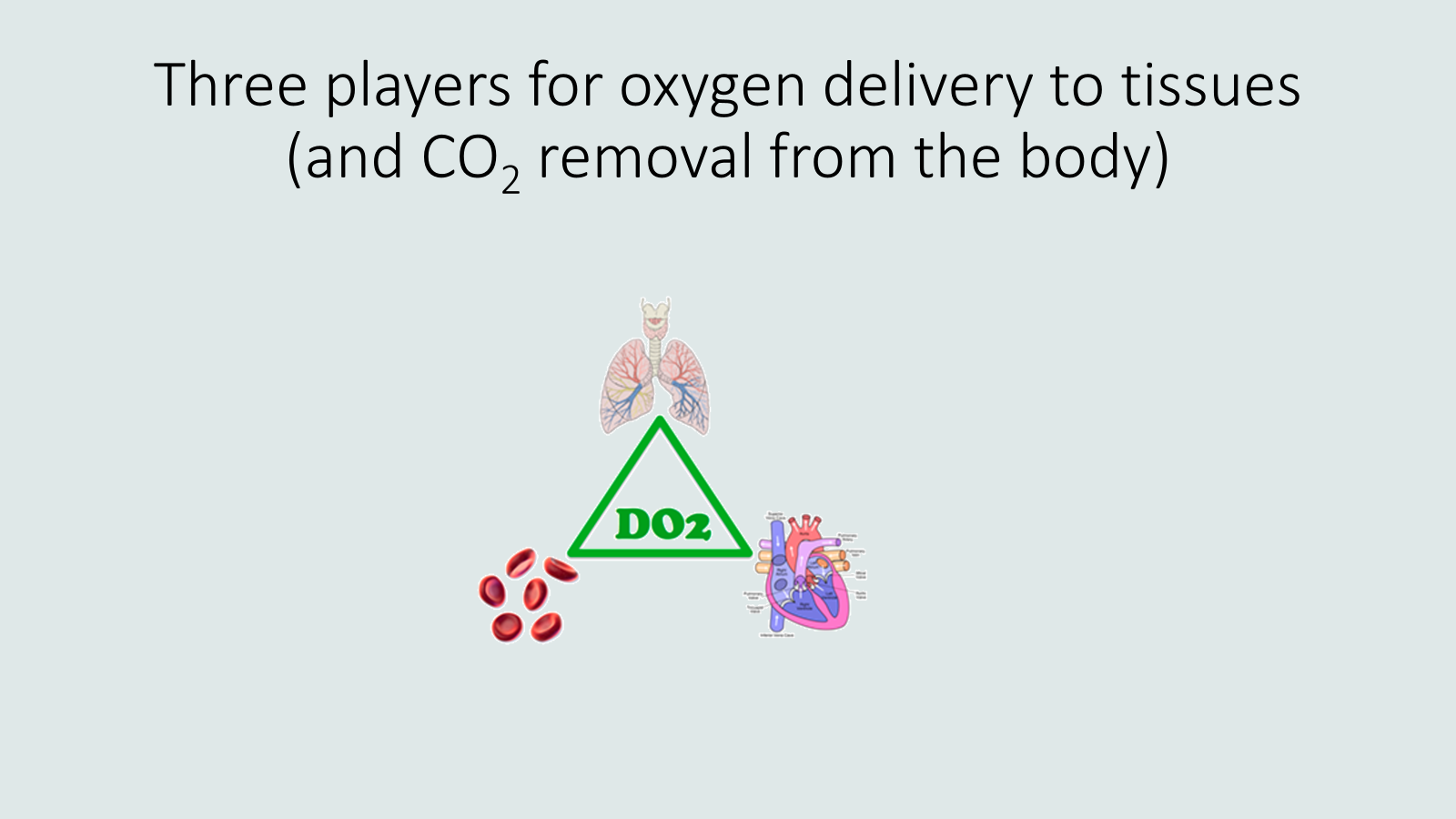
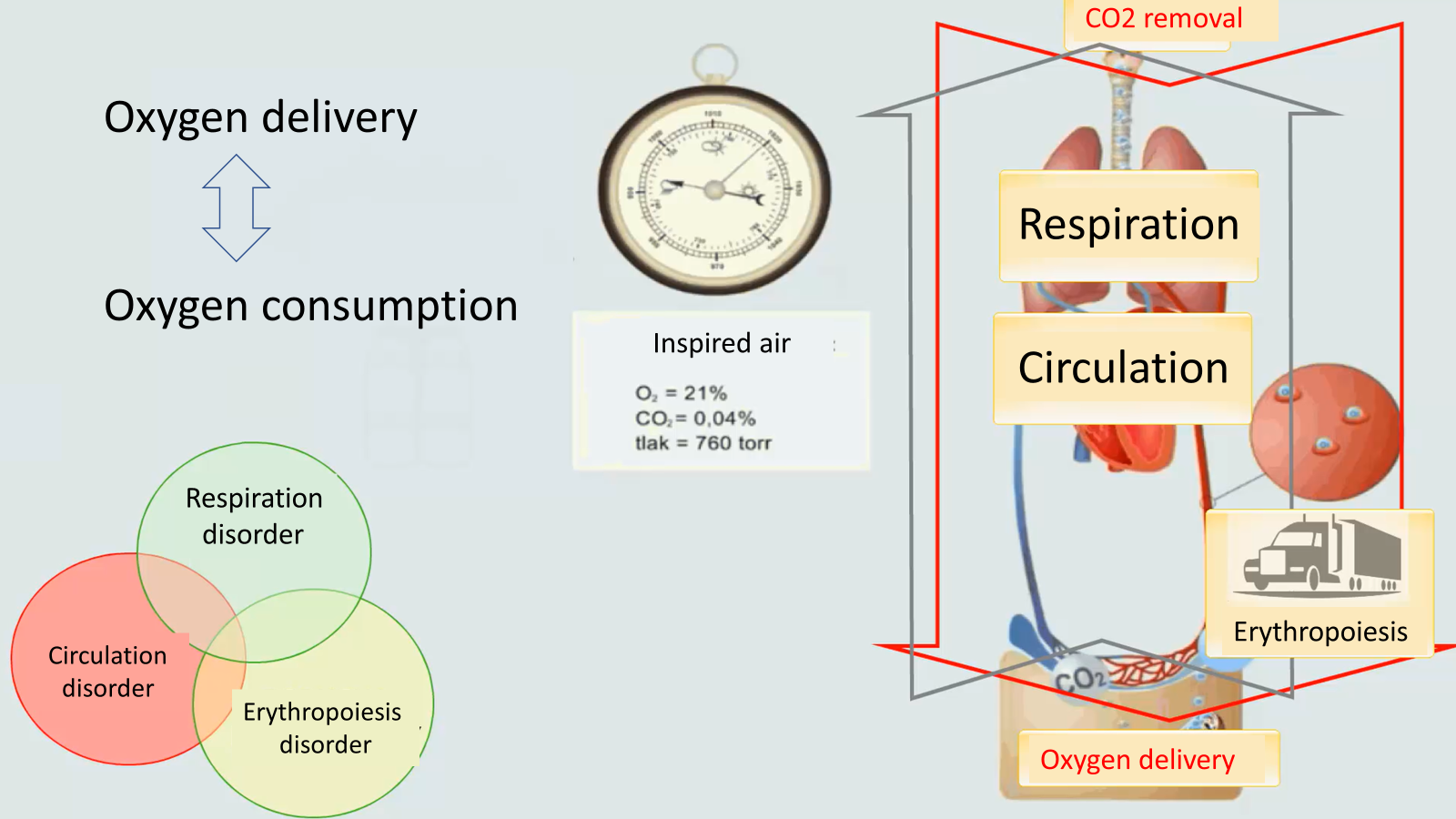
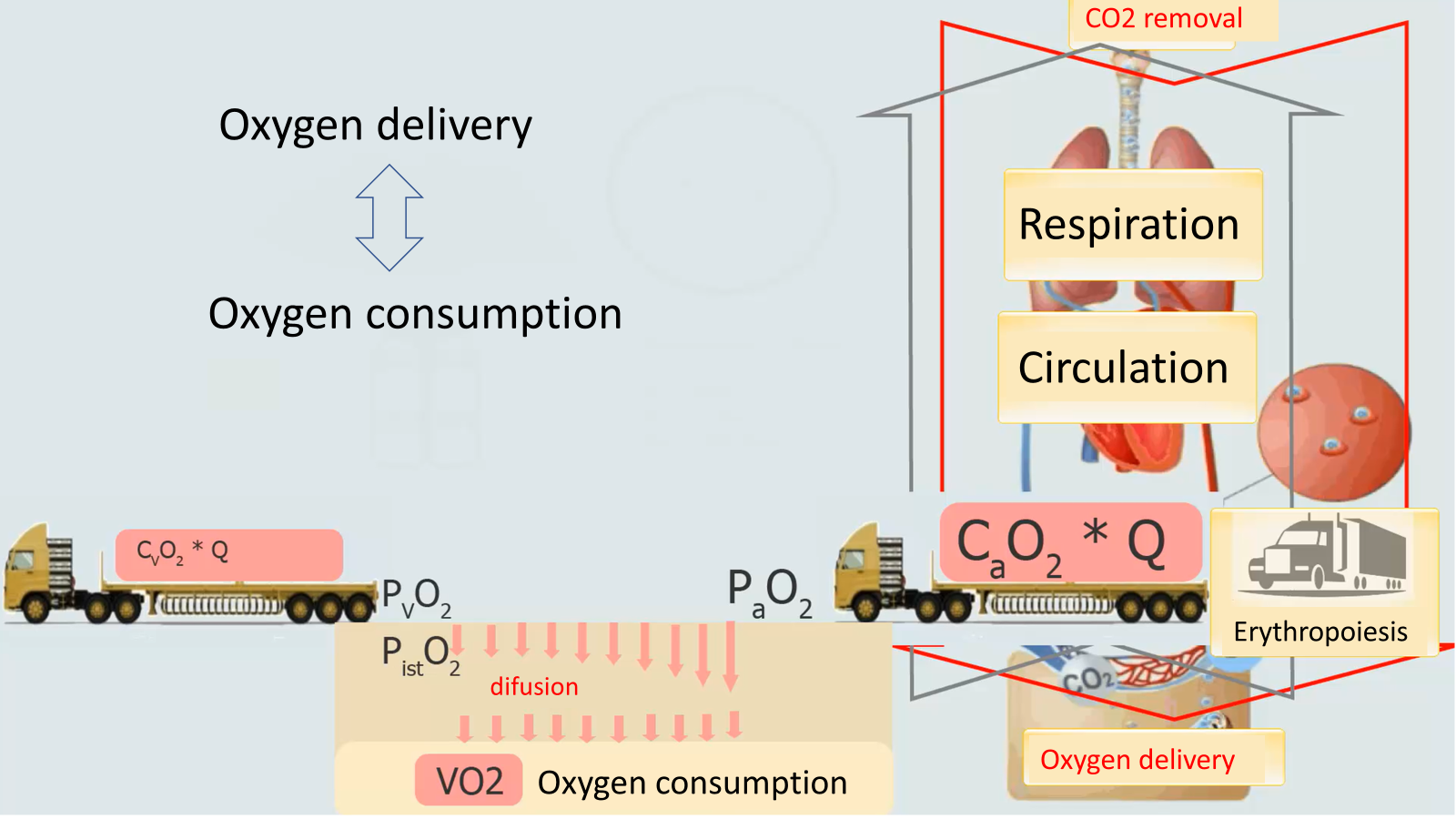
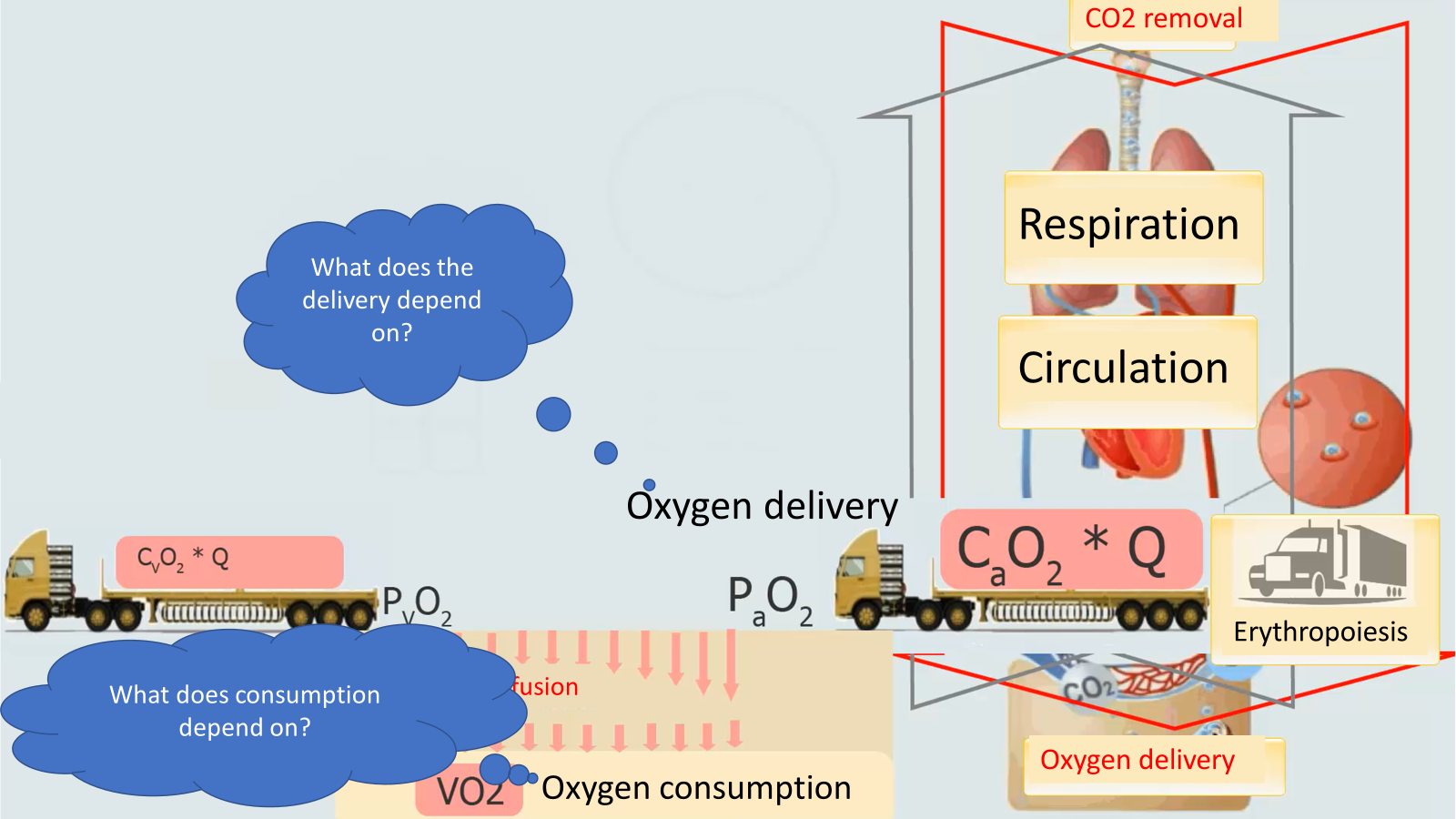
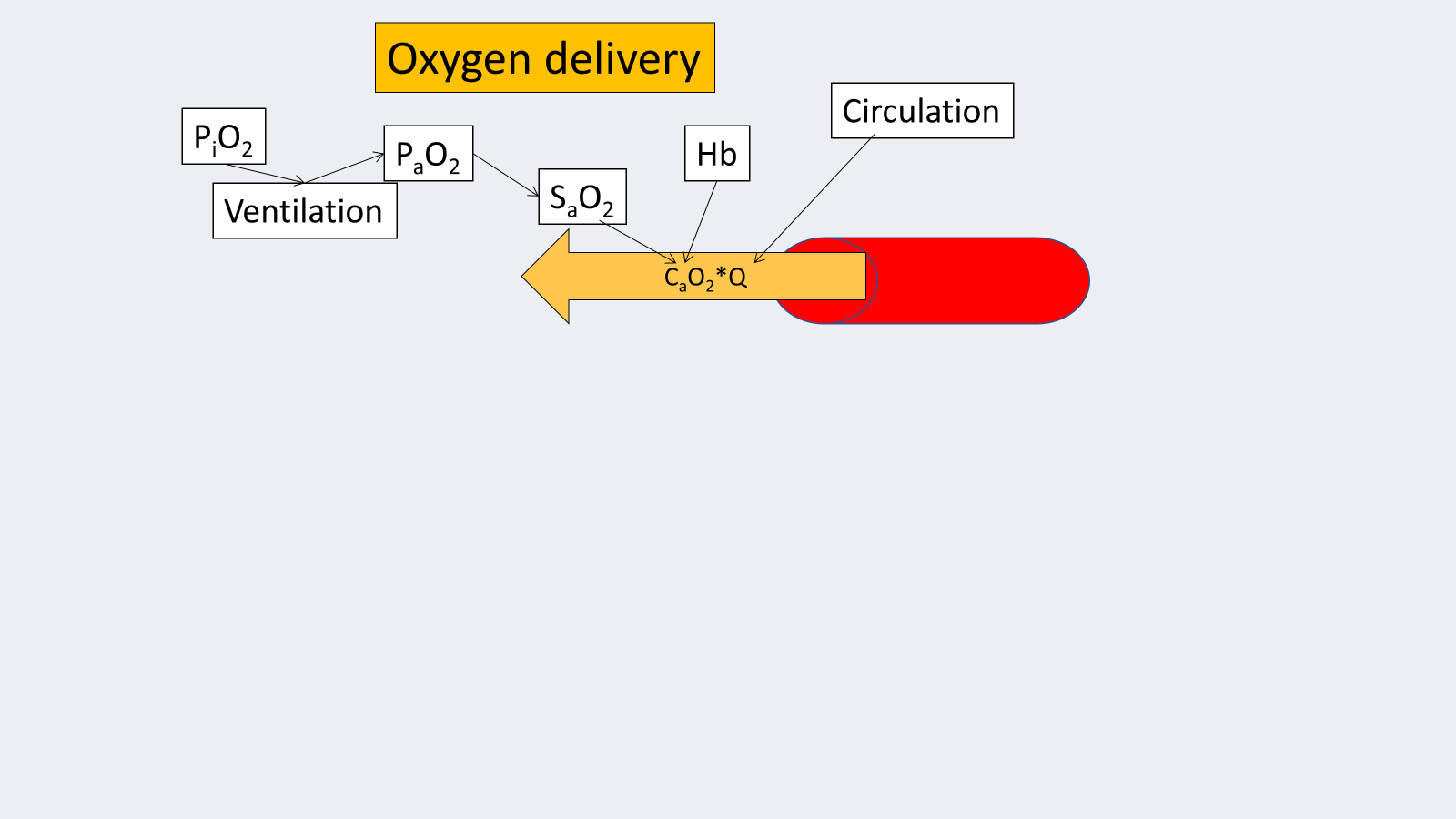
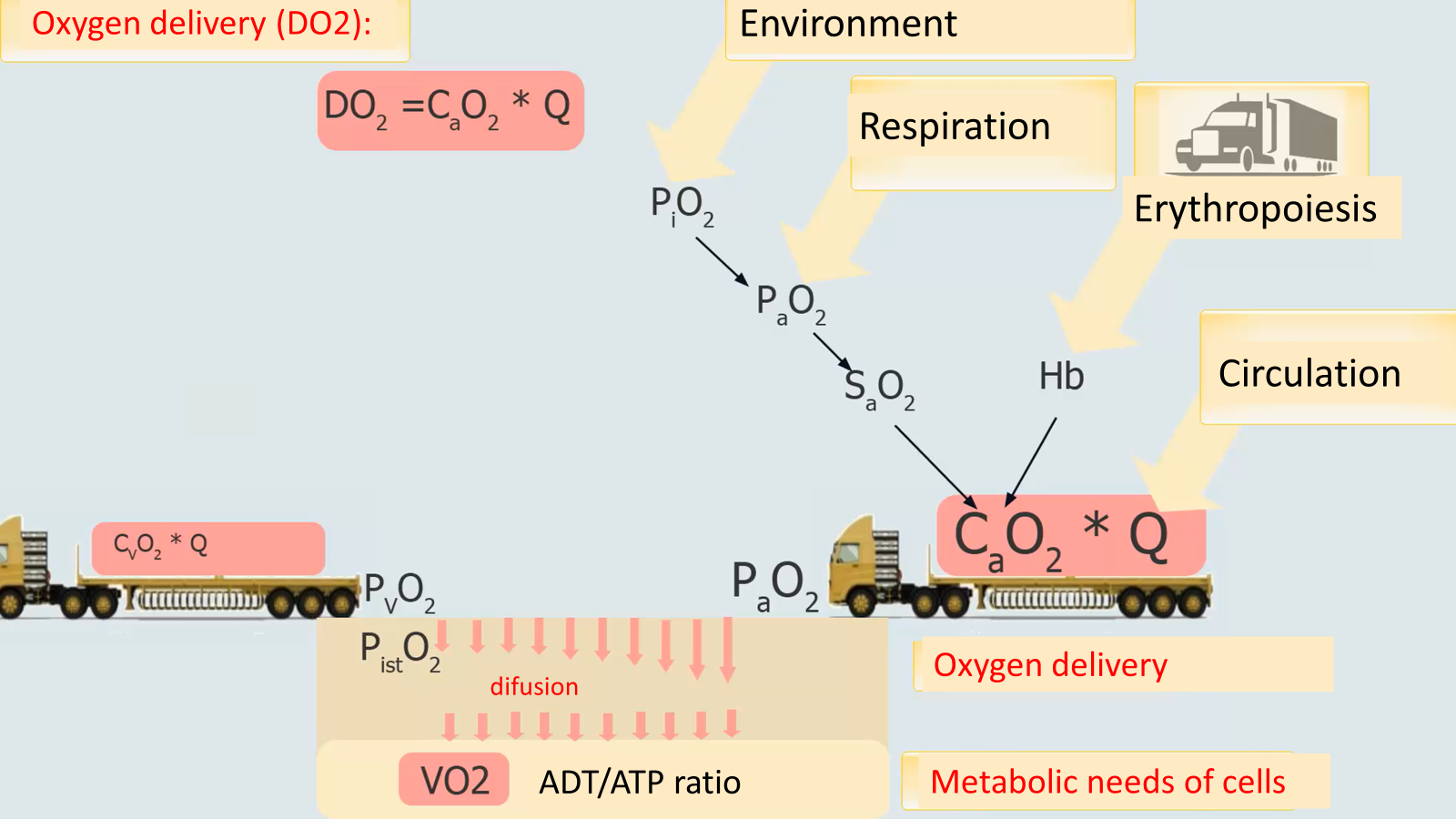
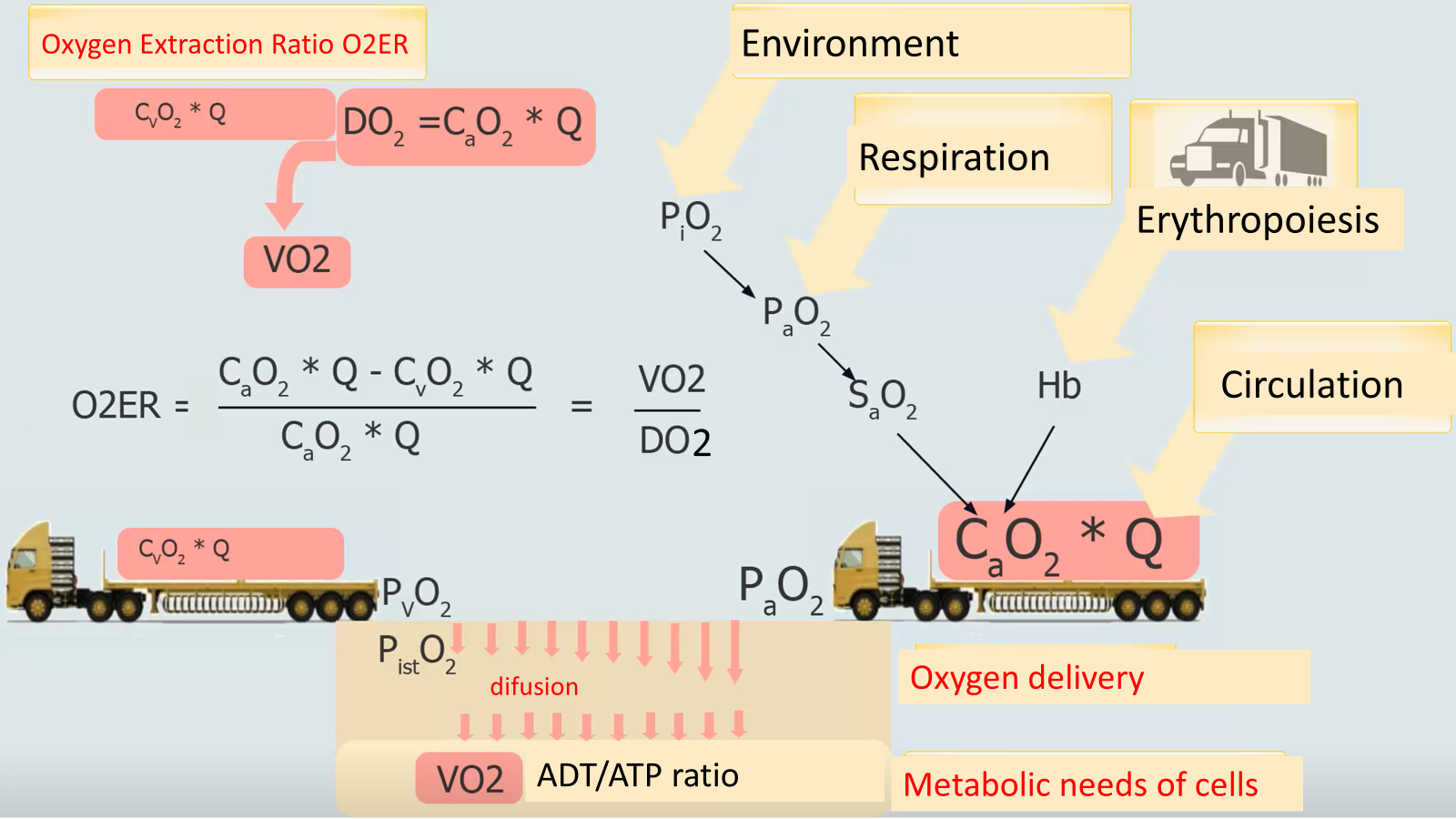
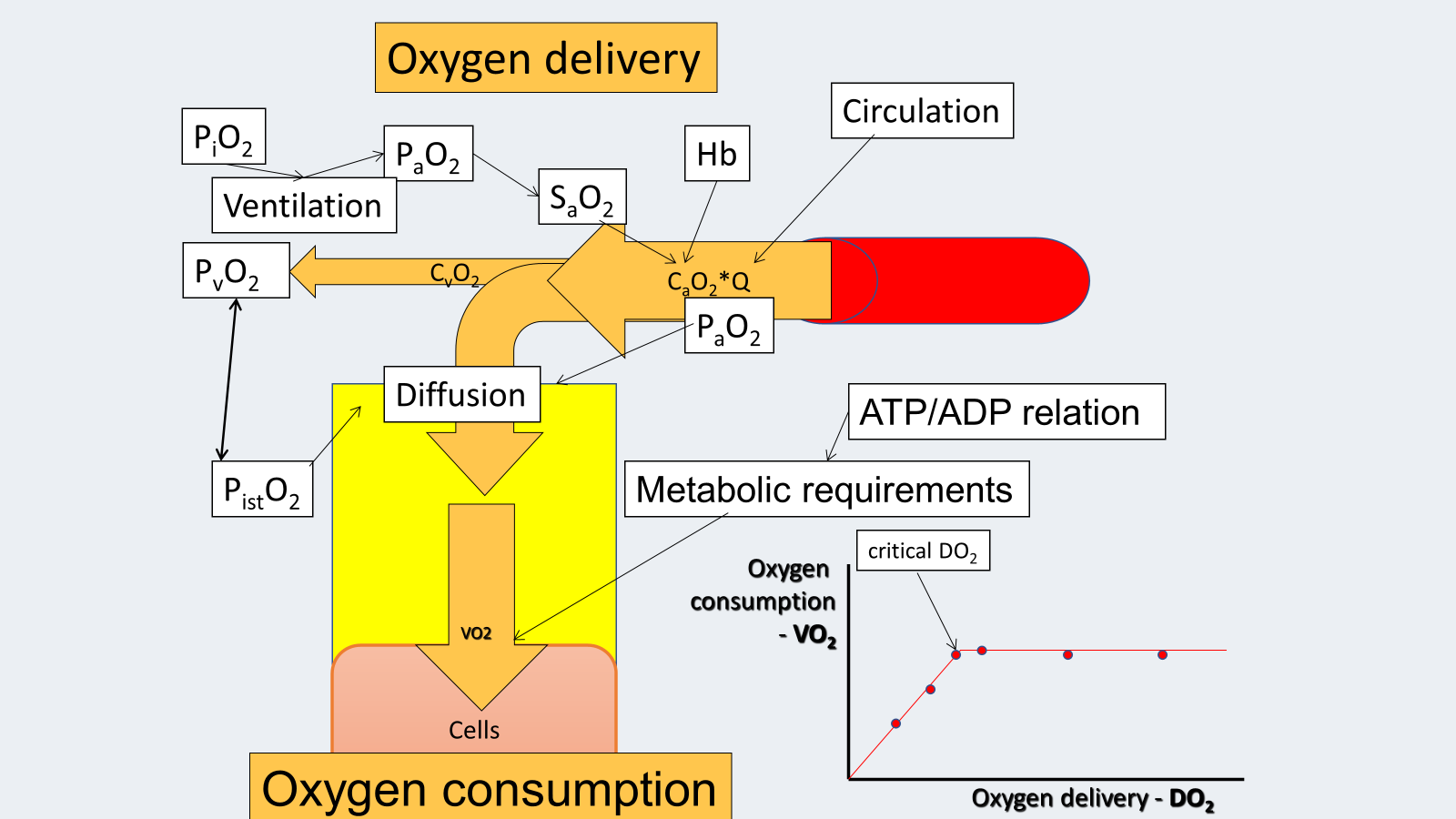
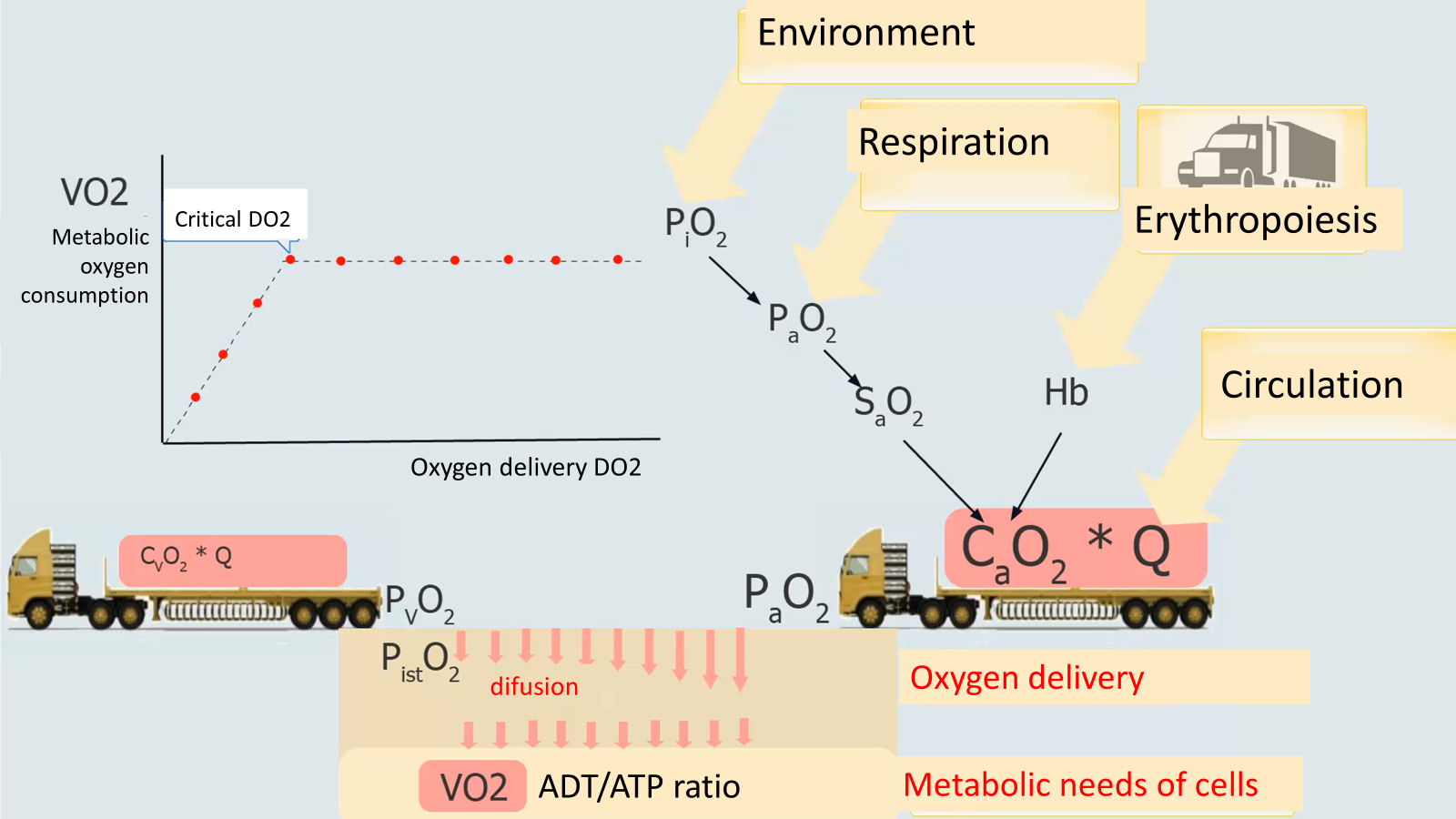
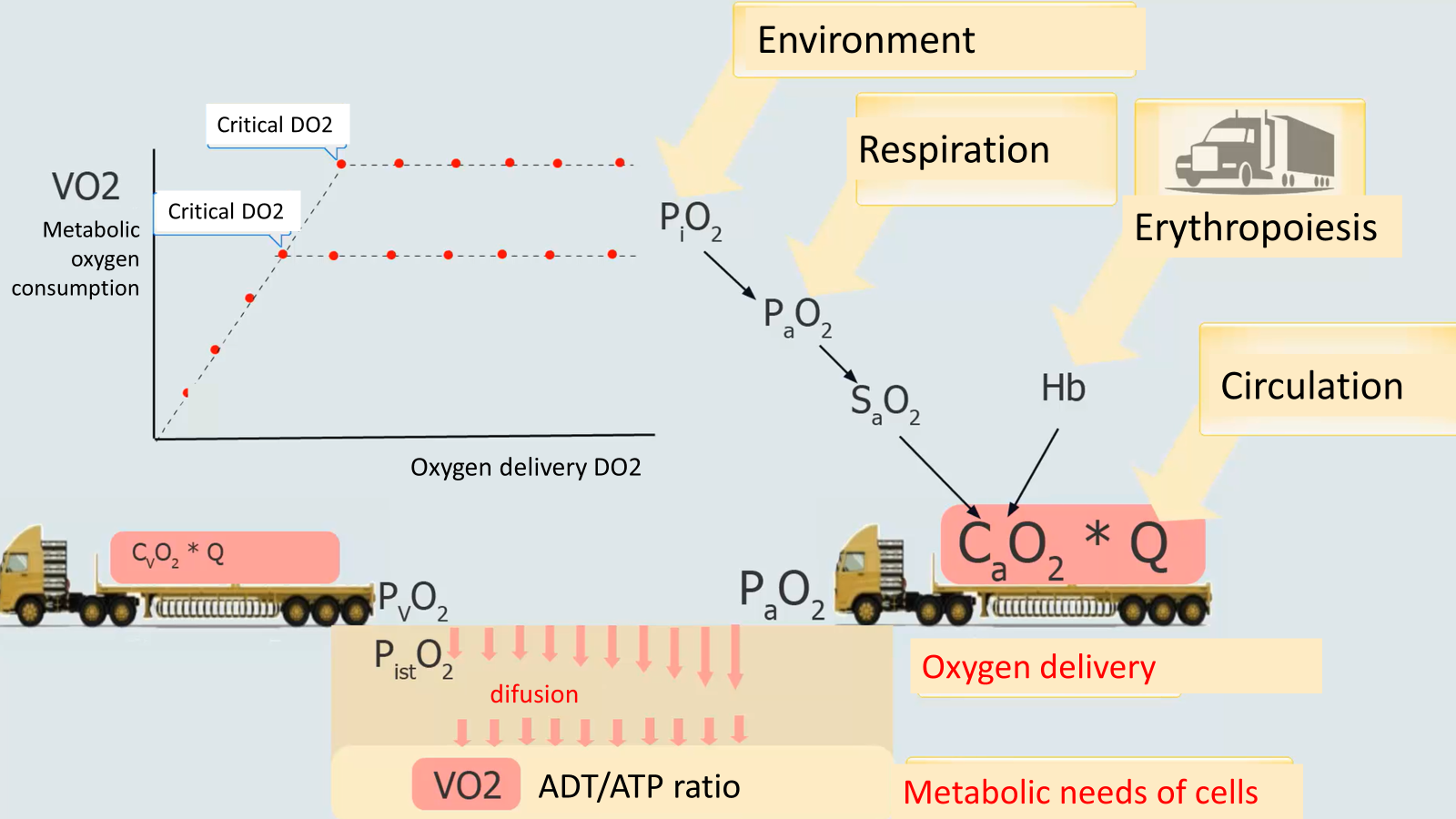
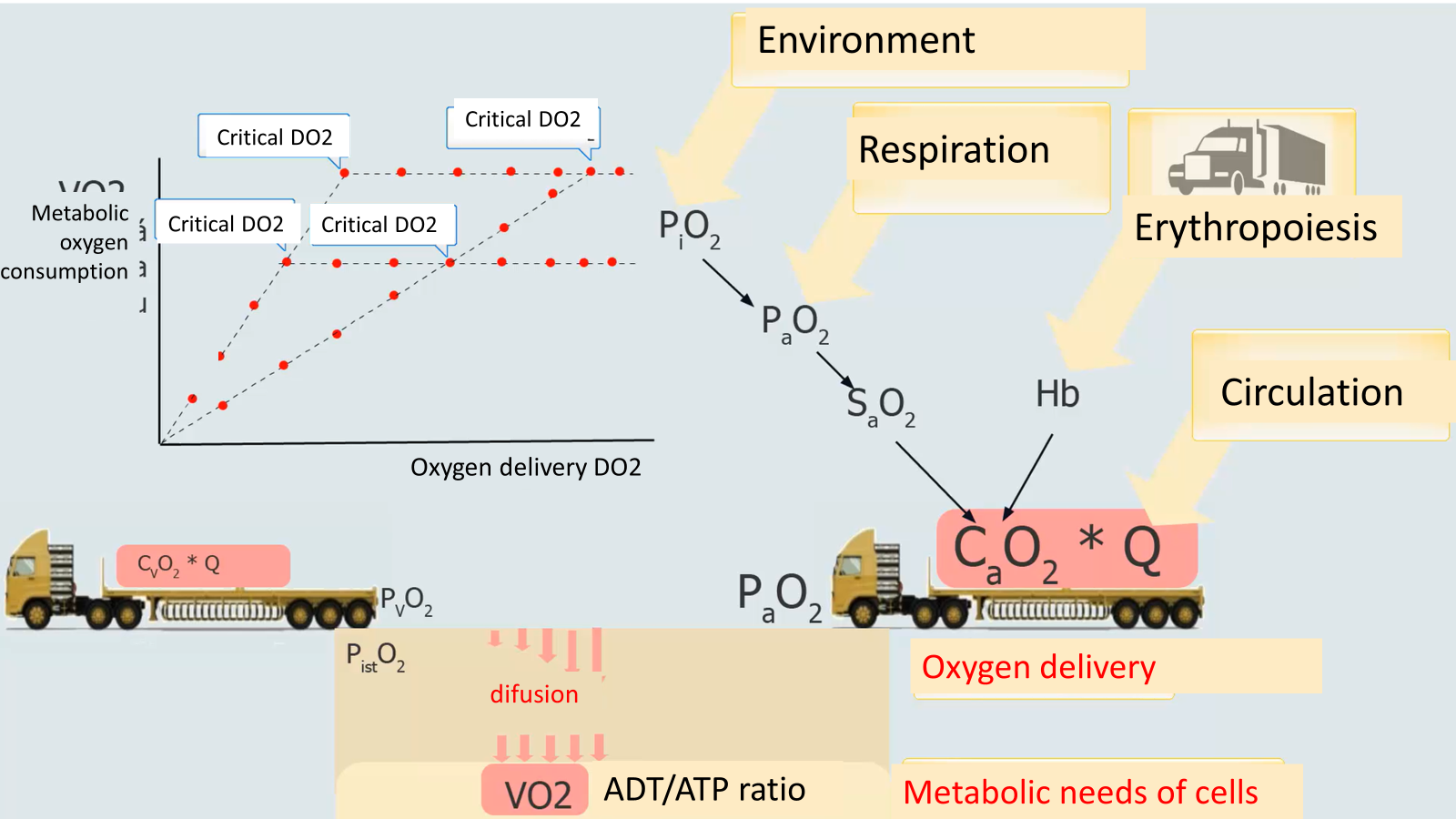
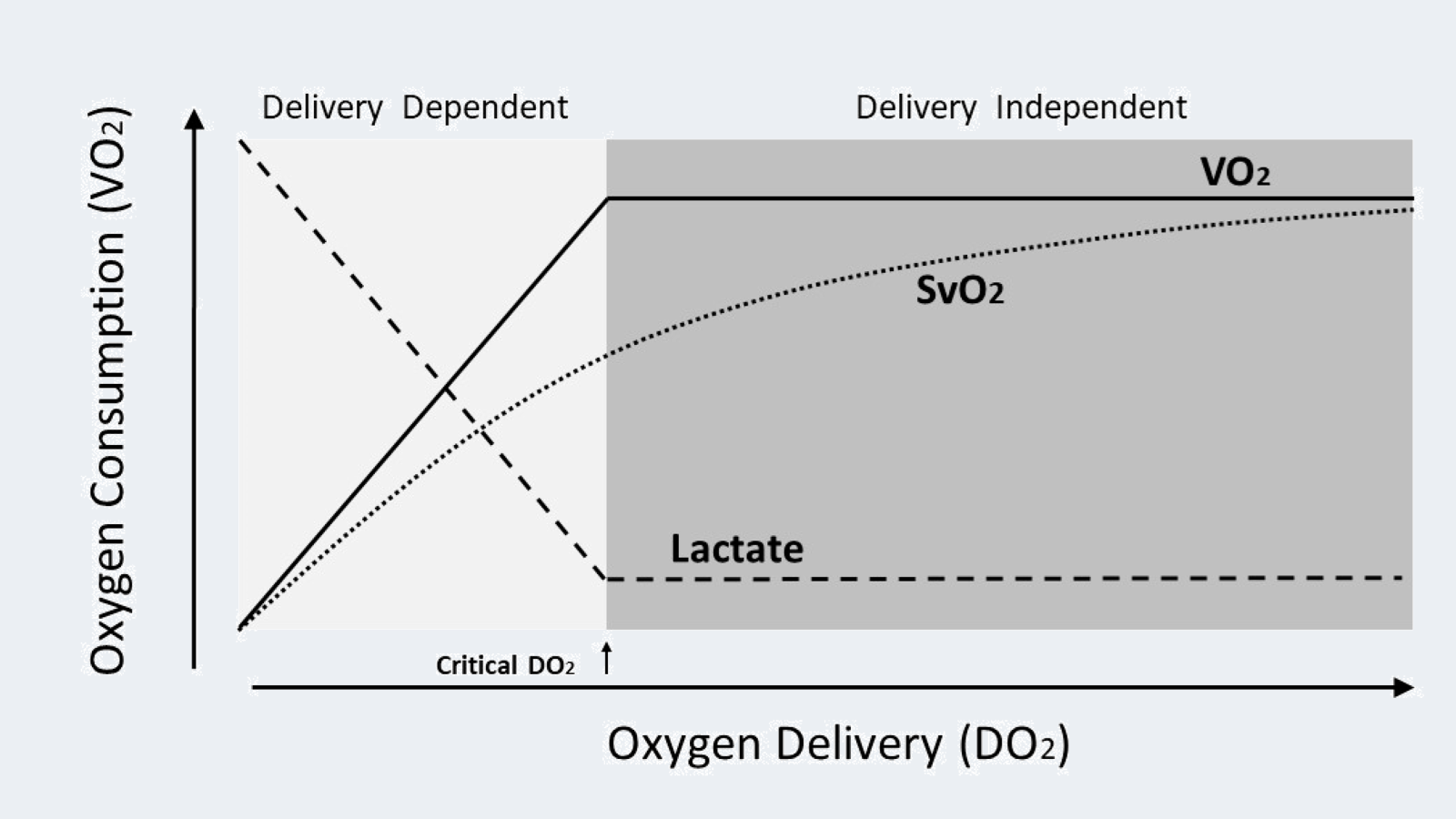
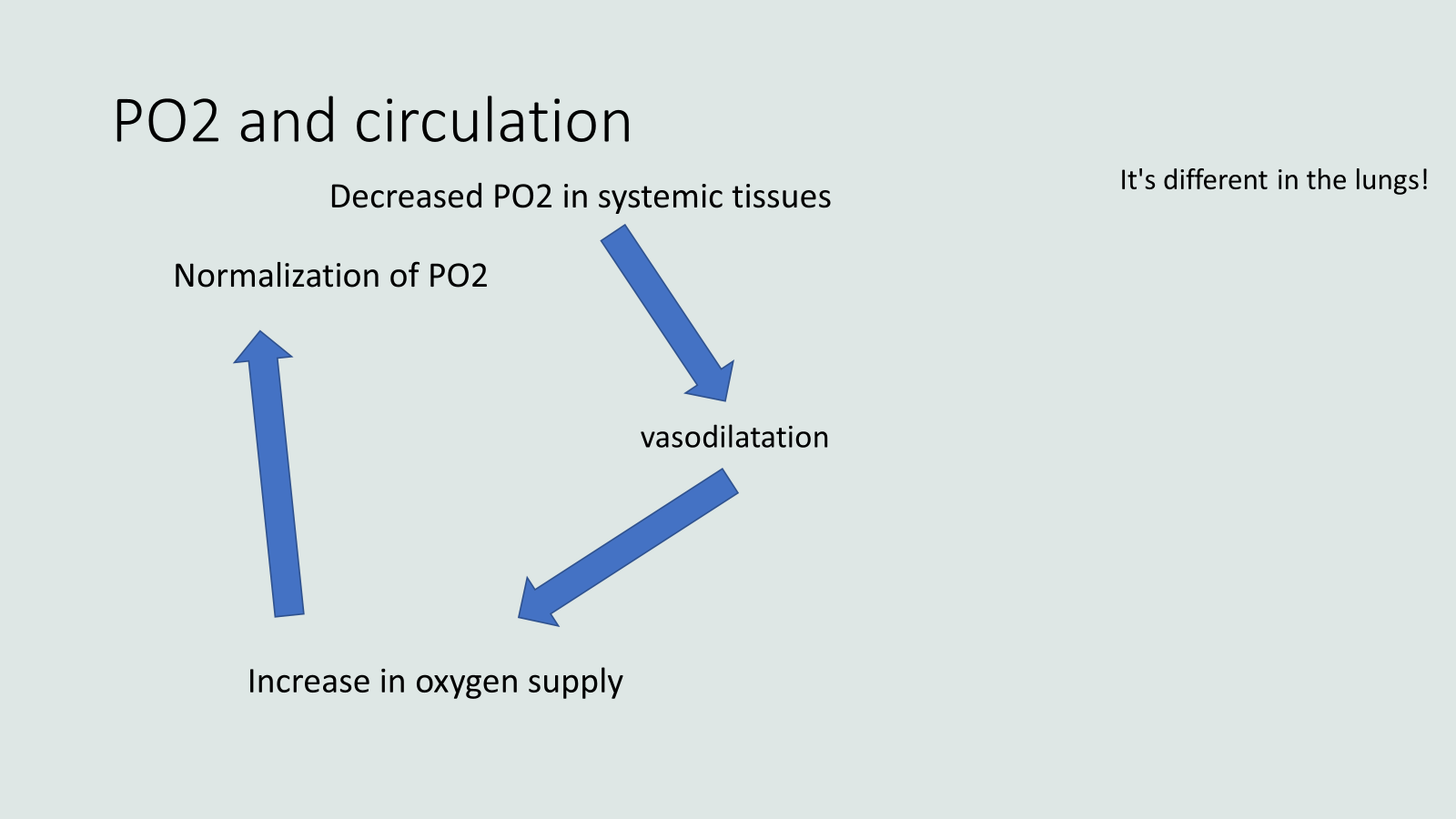
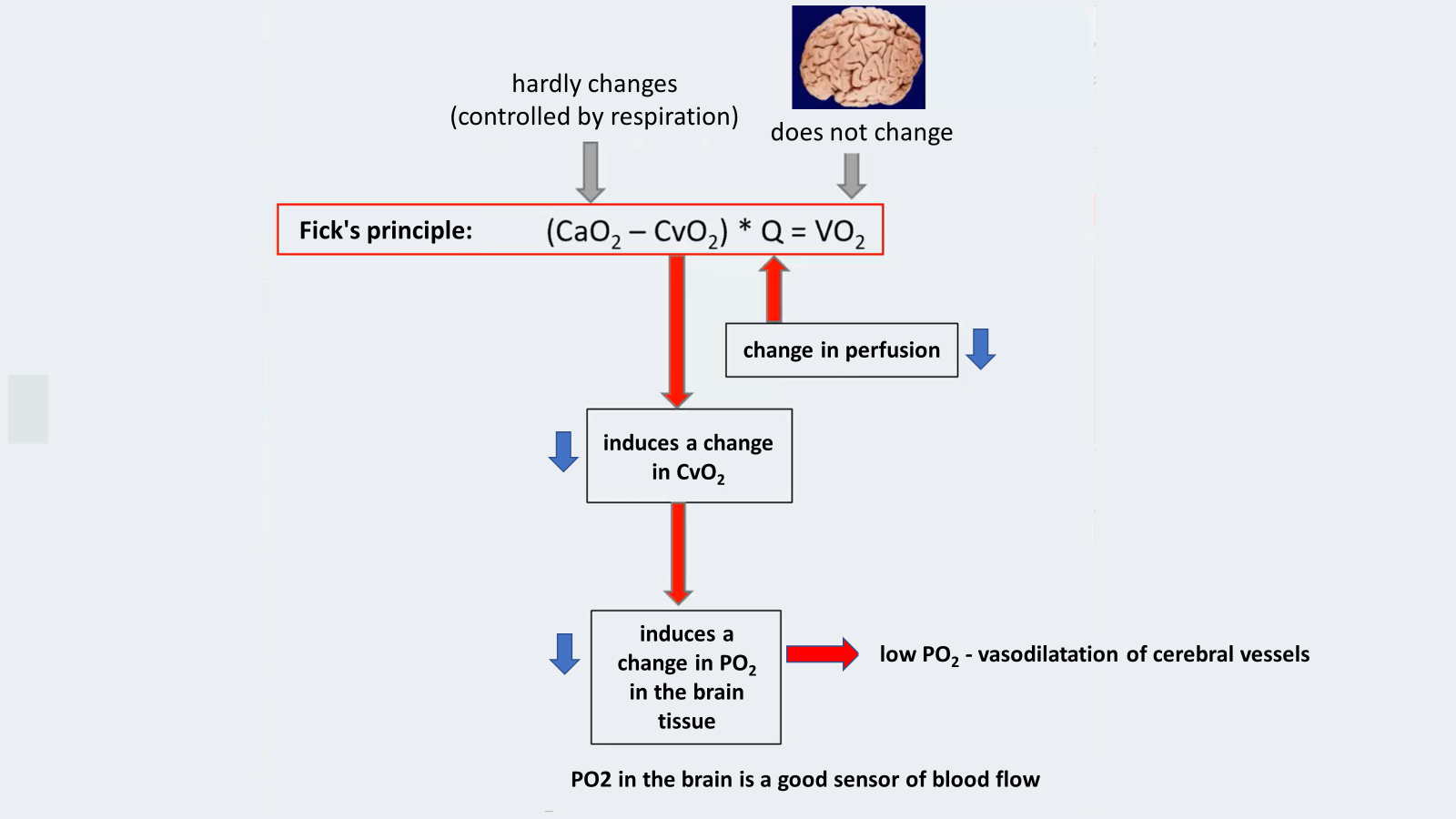
Oxygen delivery

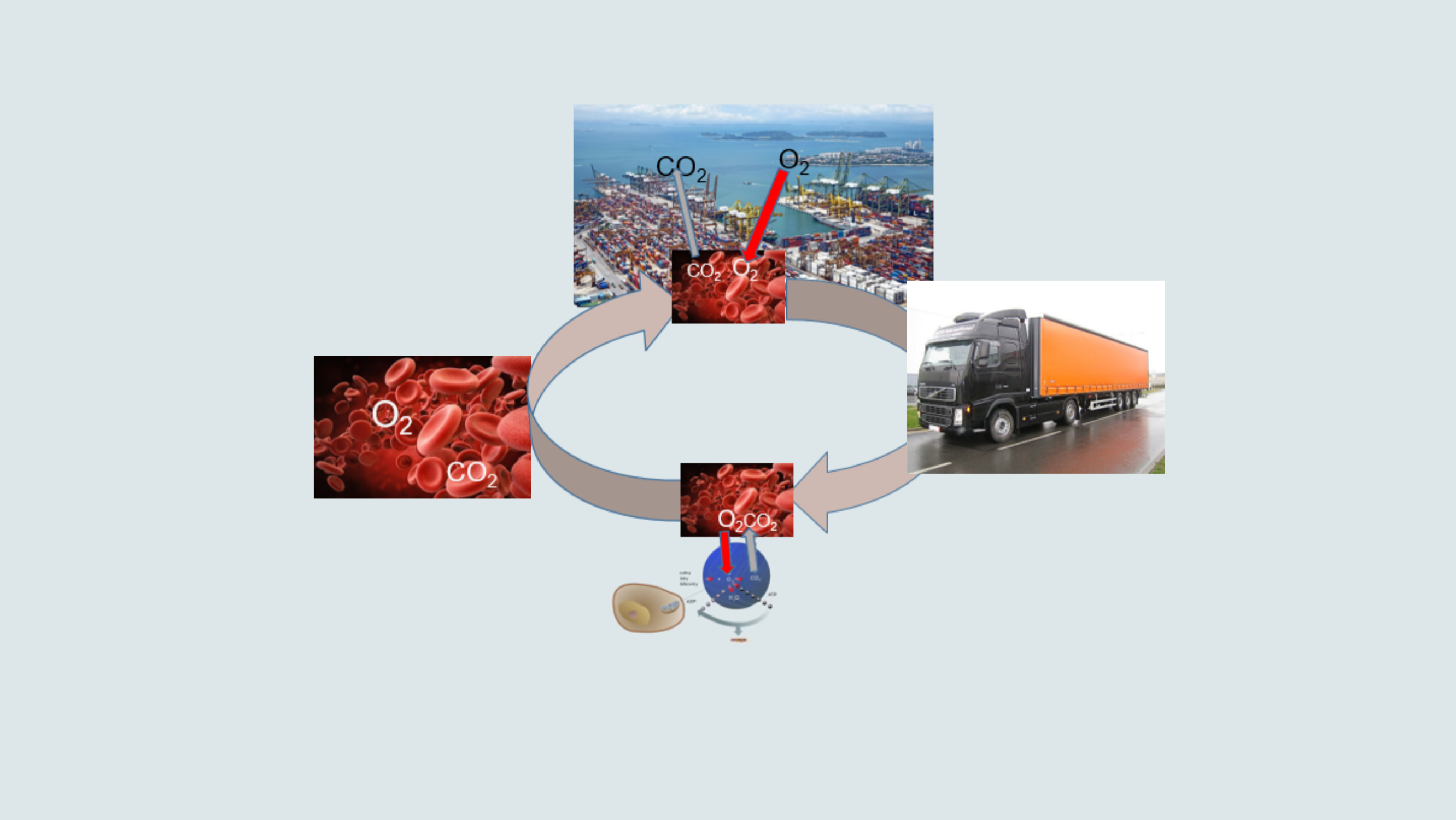
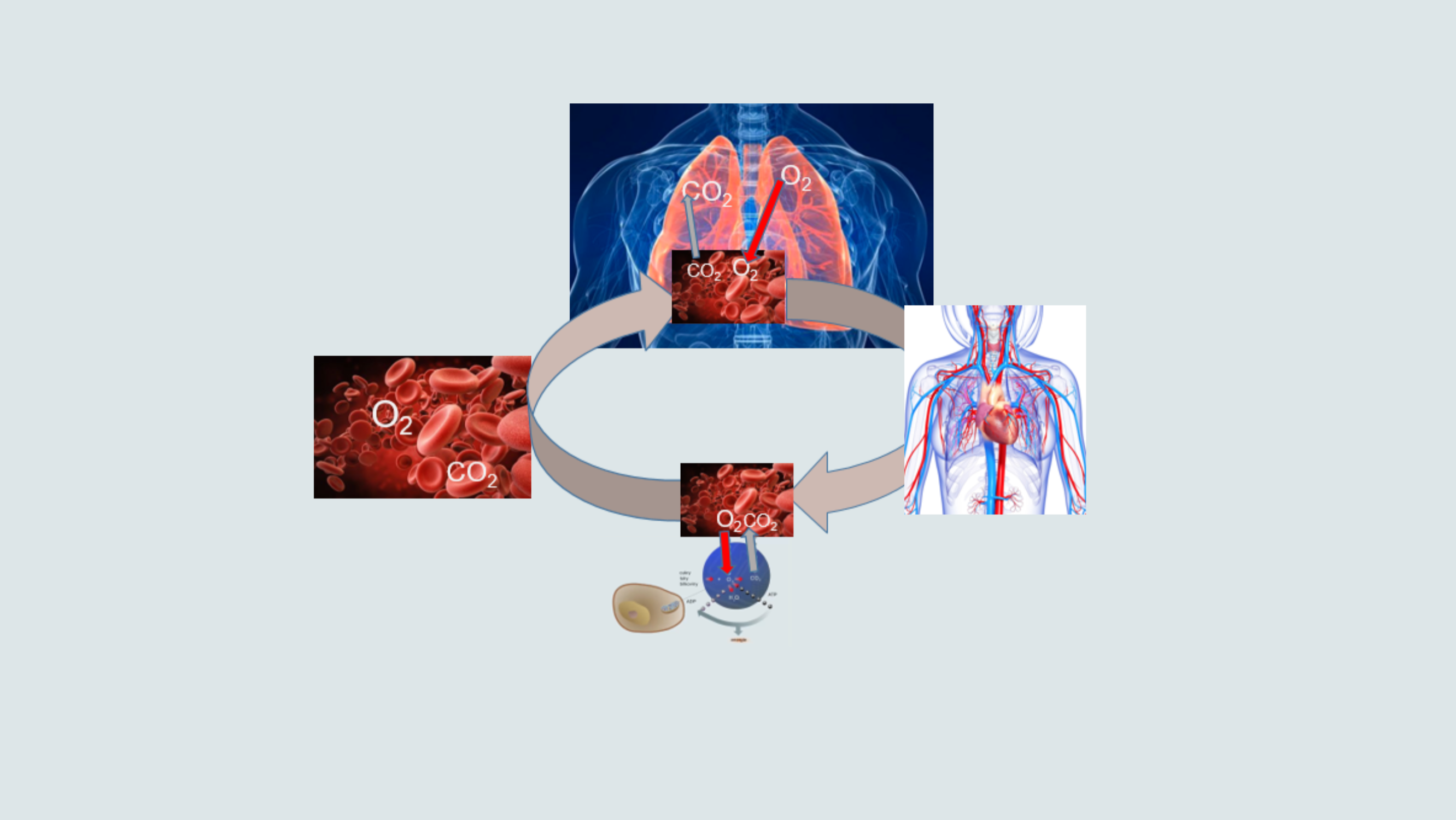
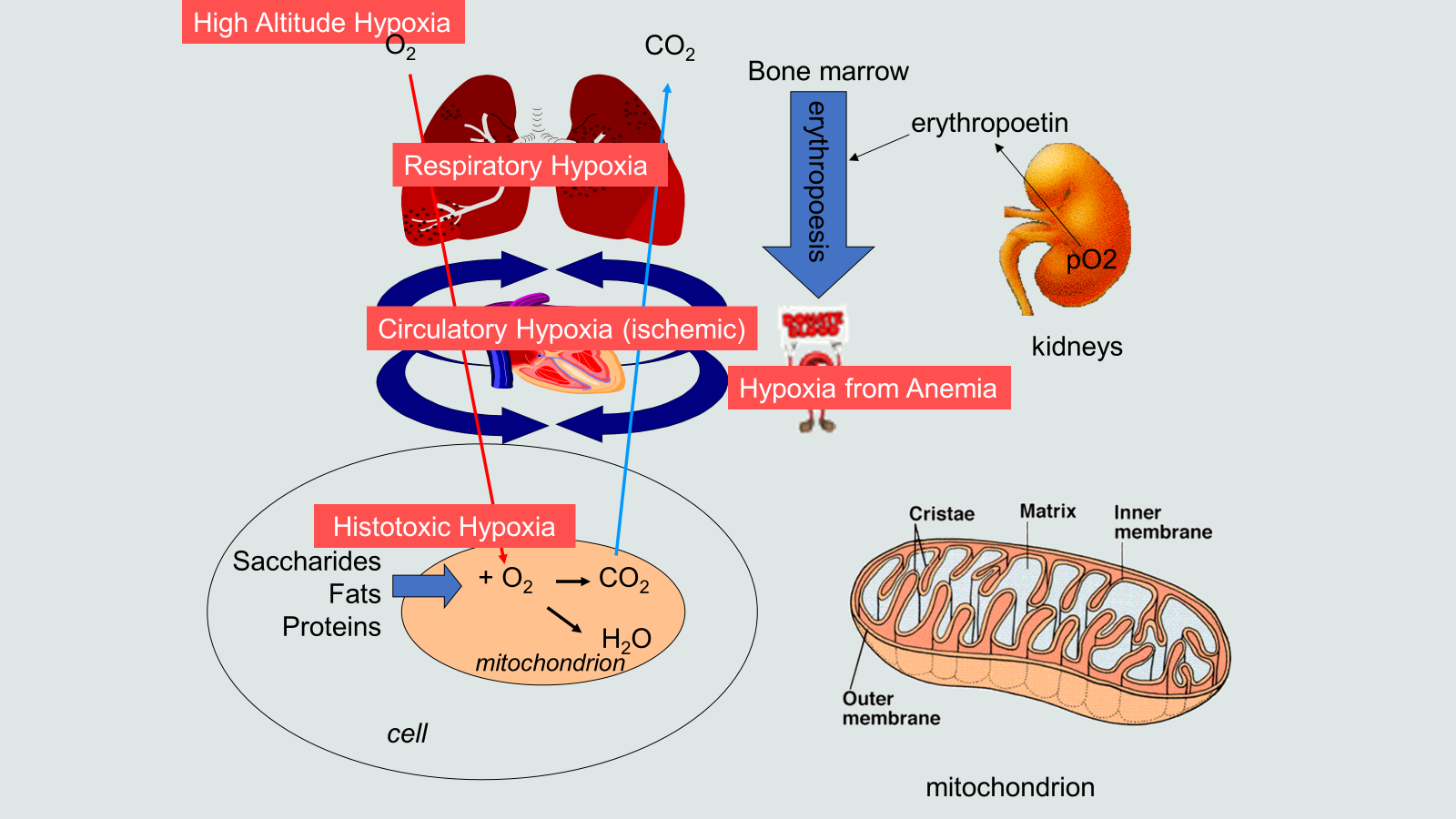
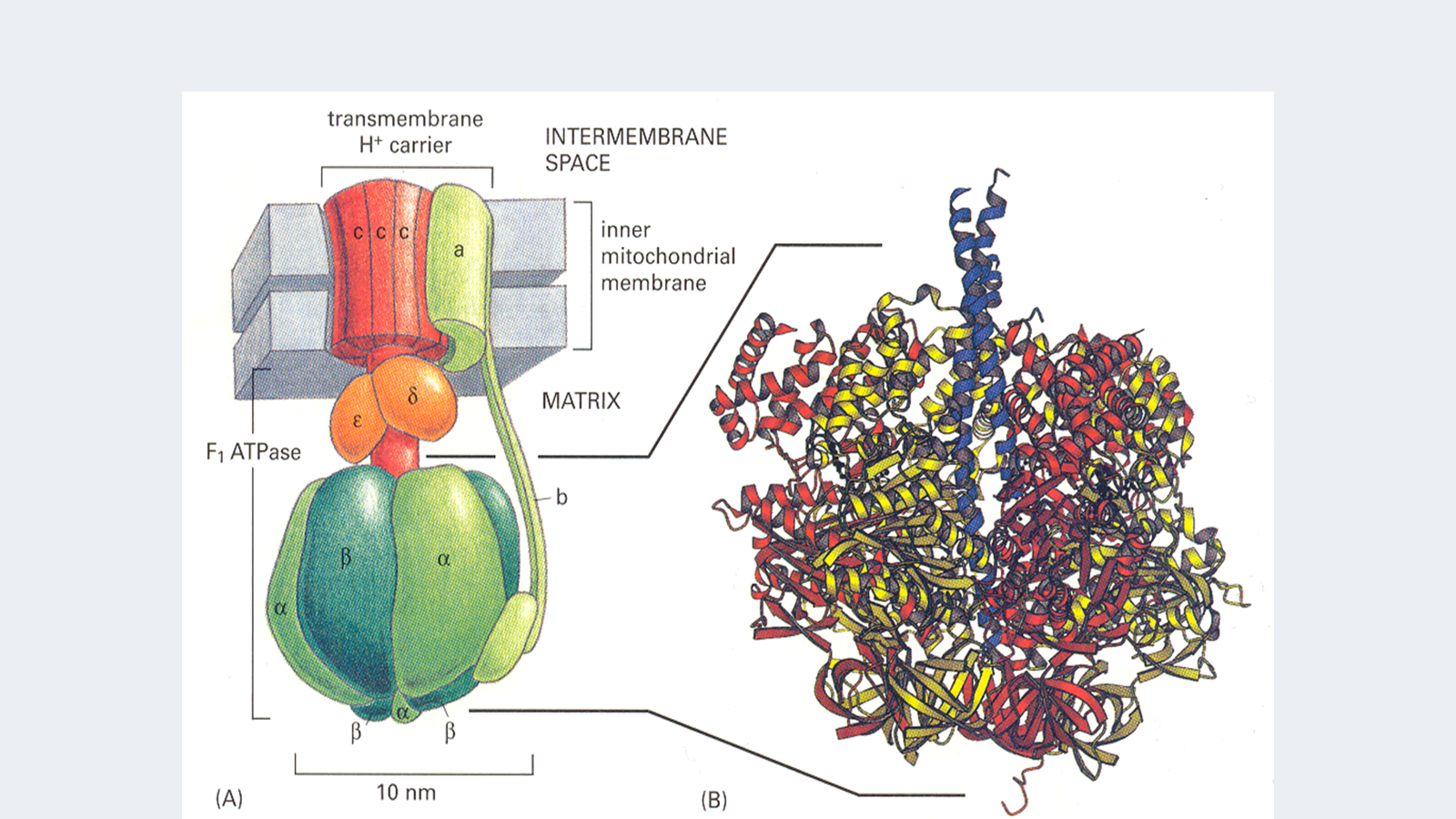
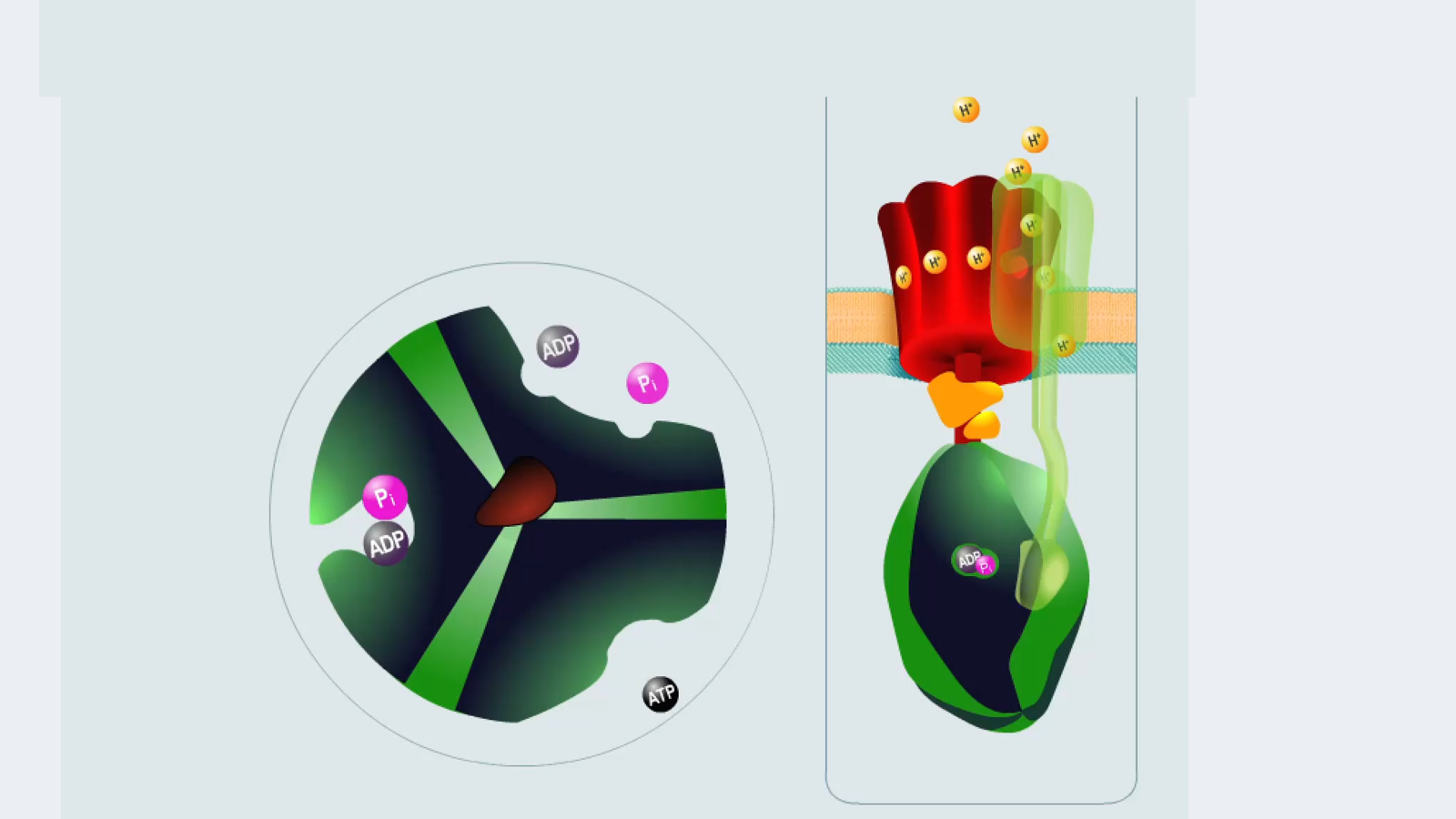
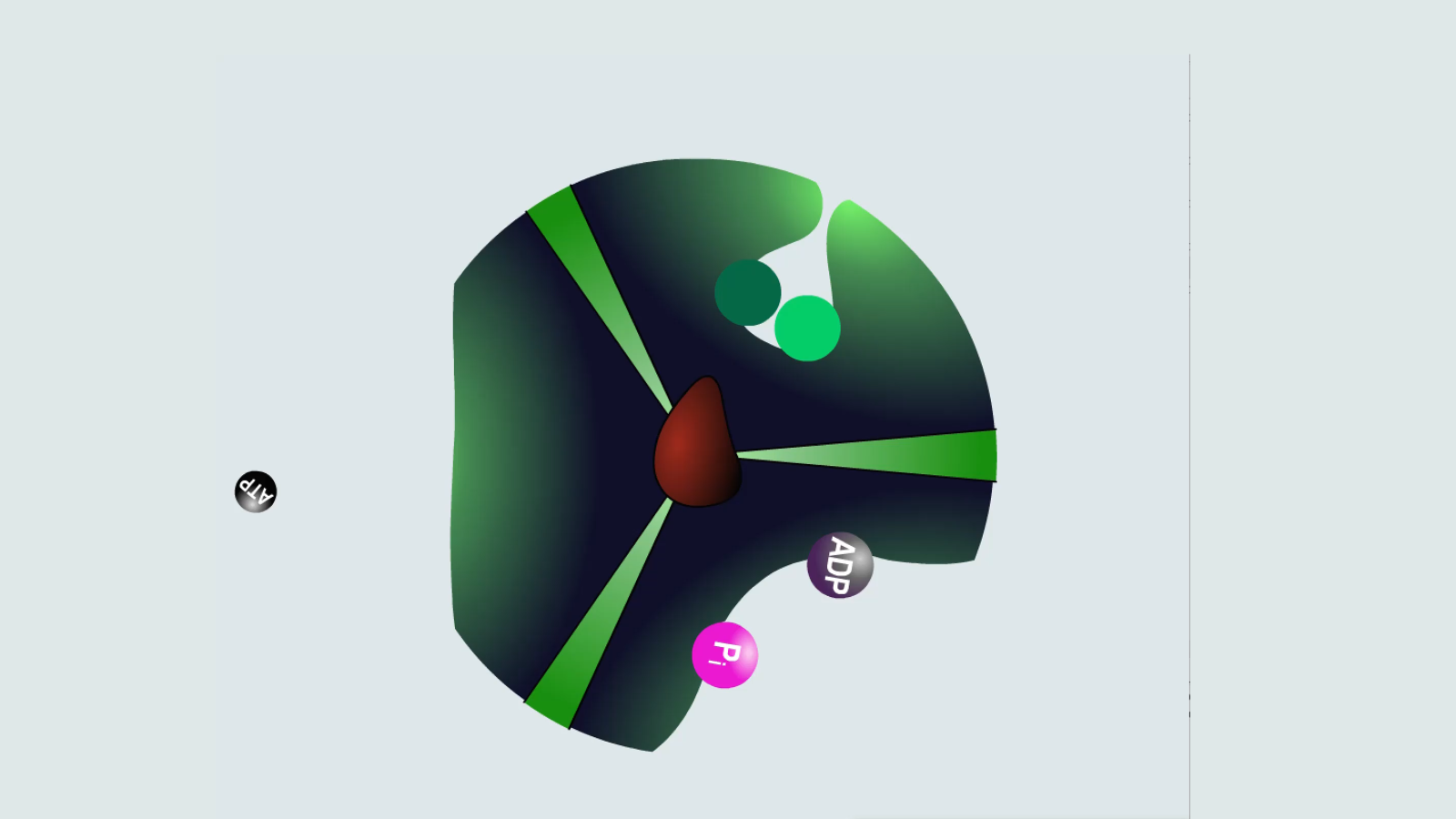
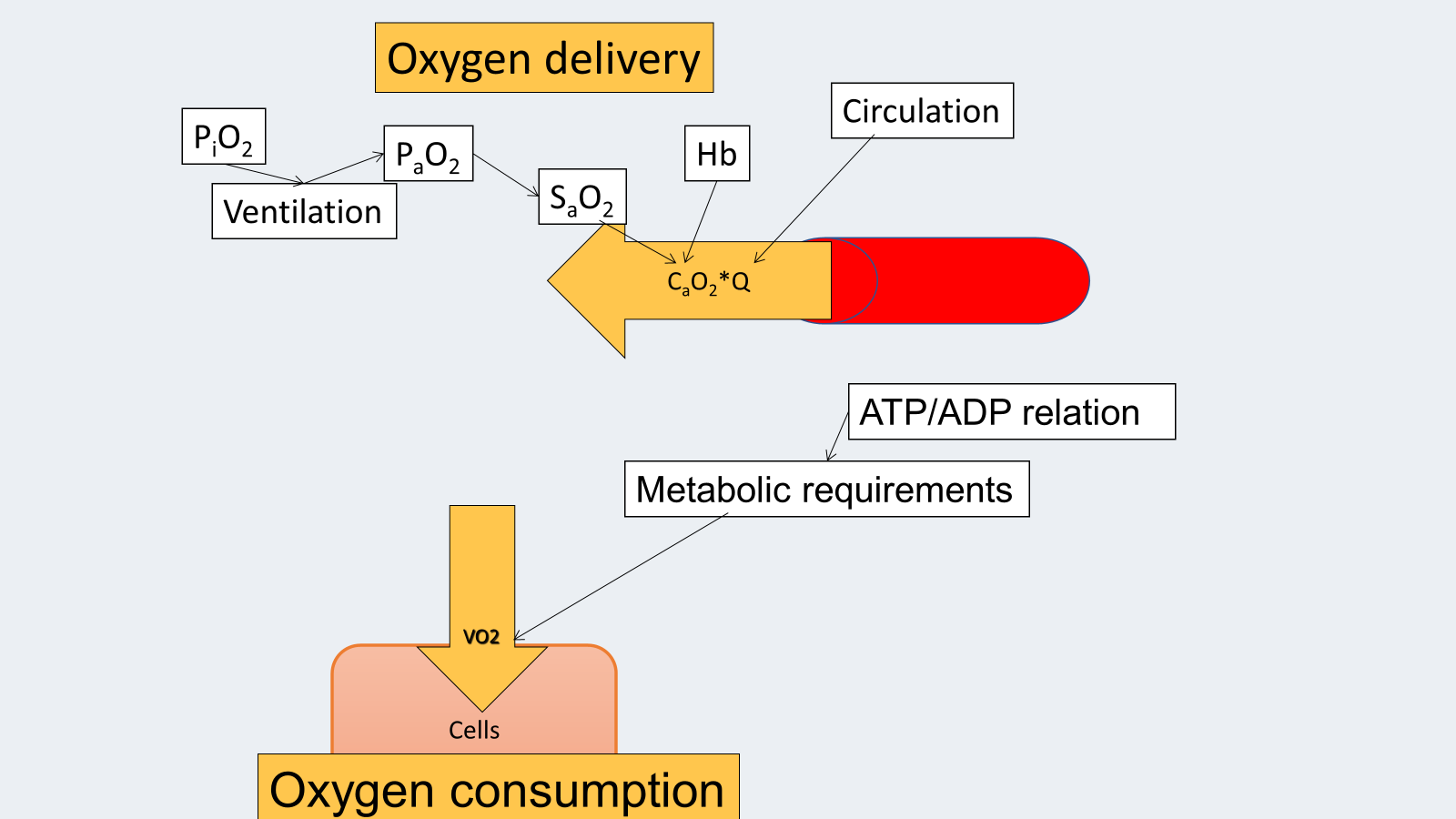
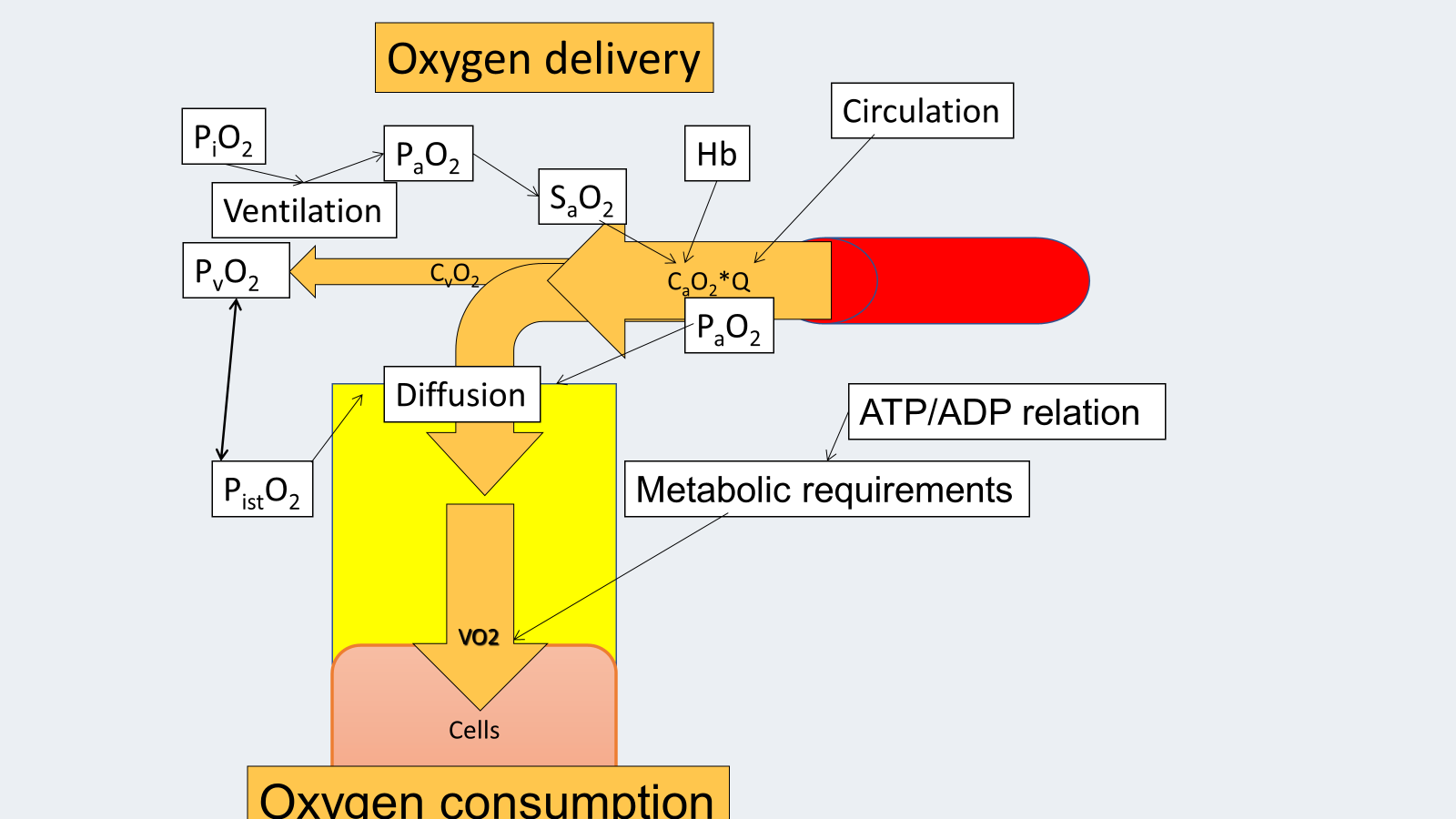
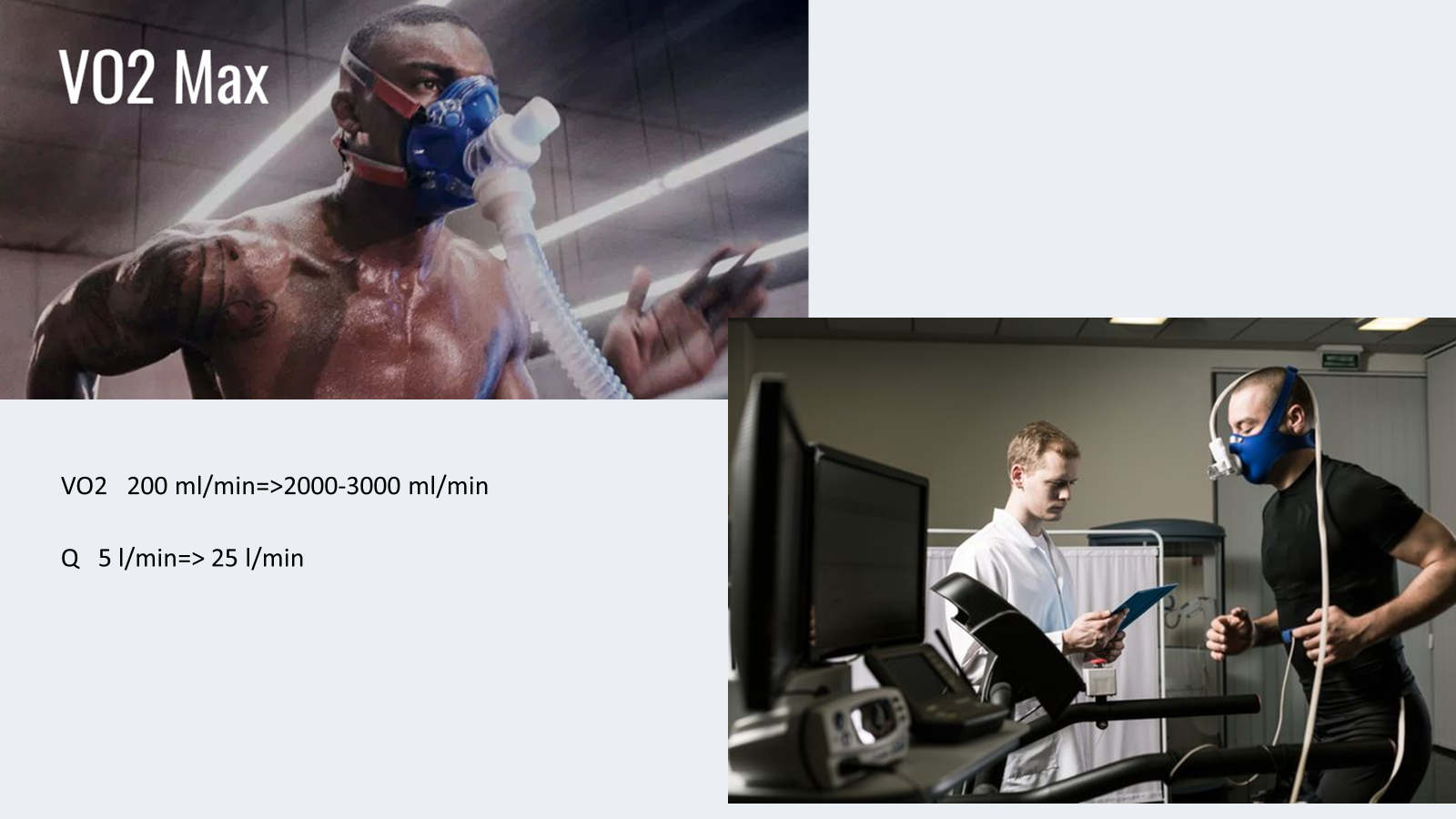
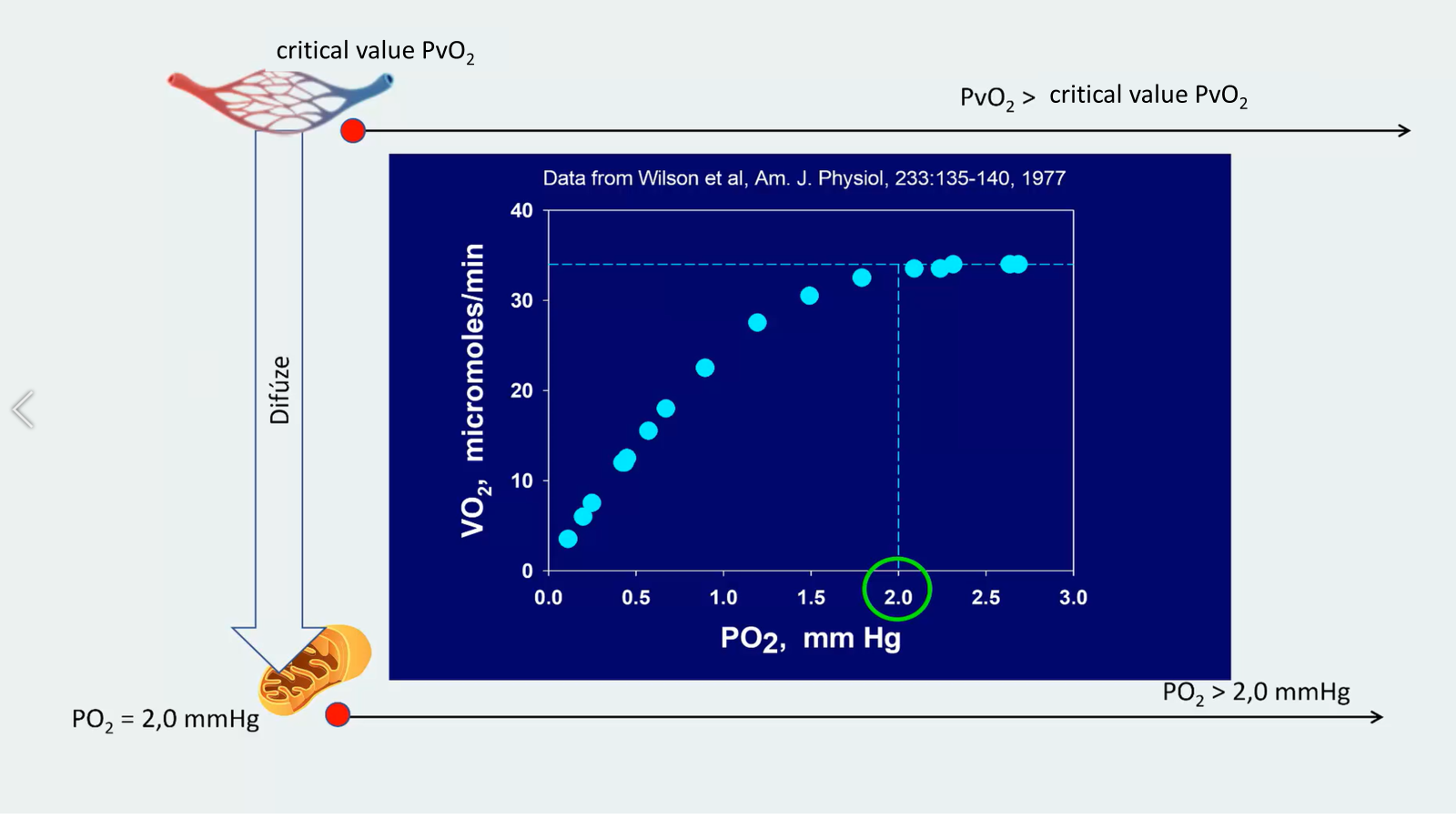
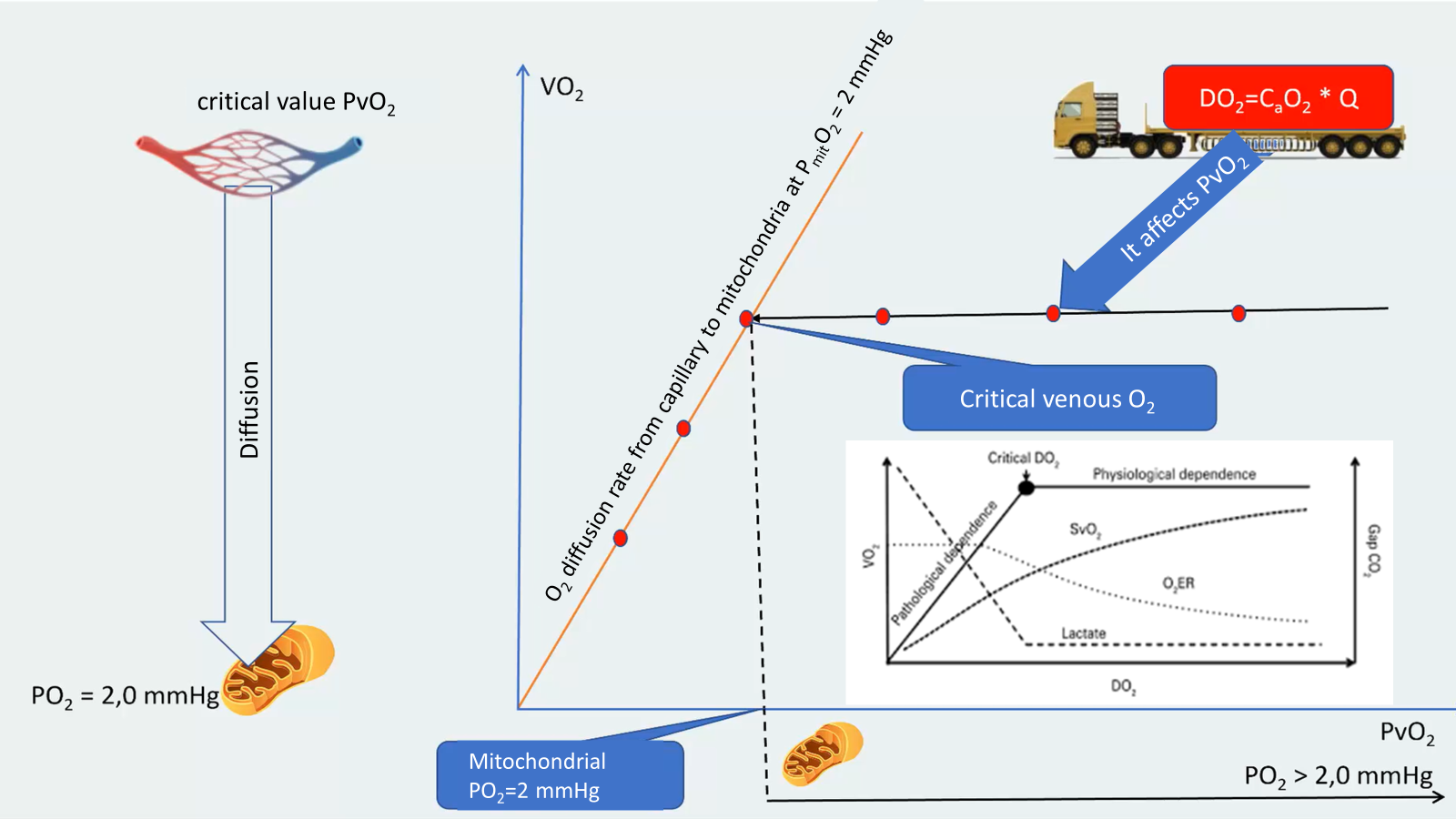
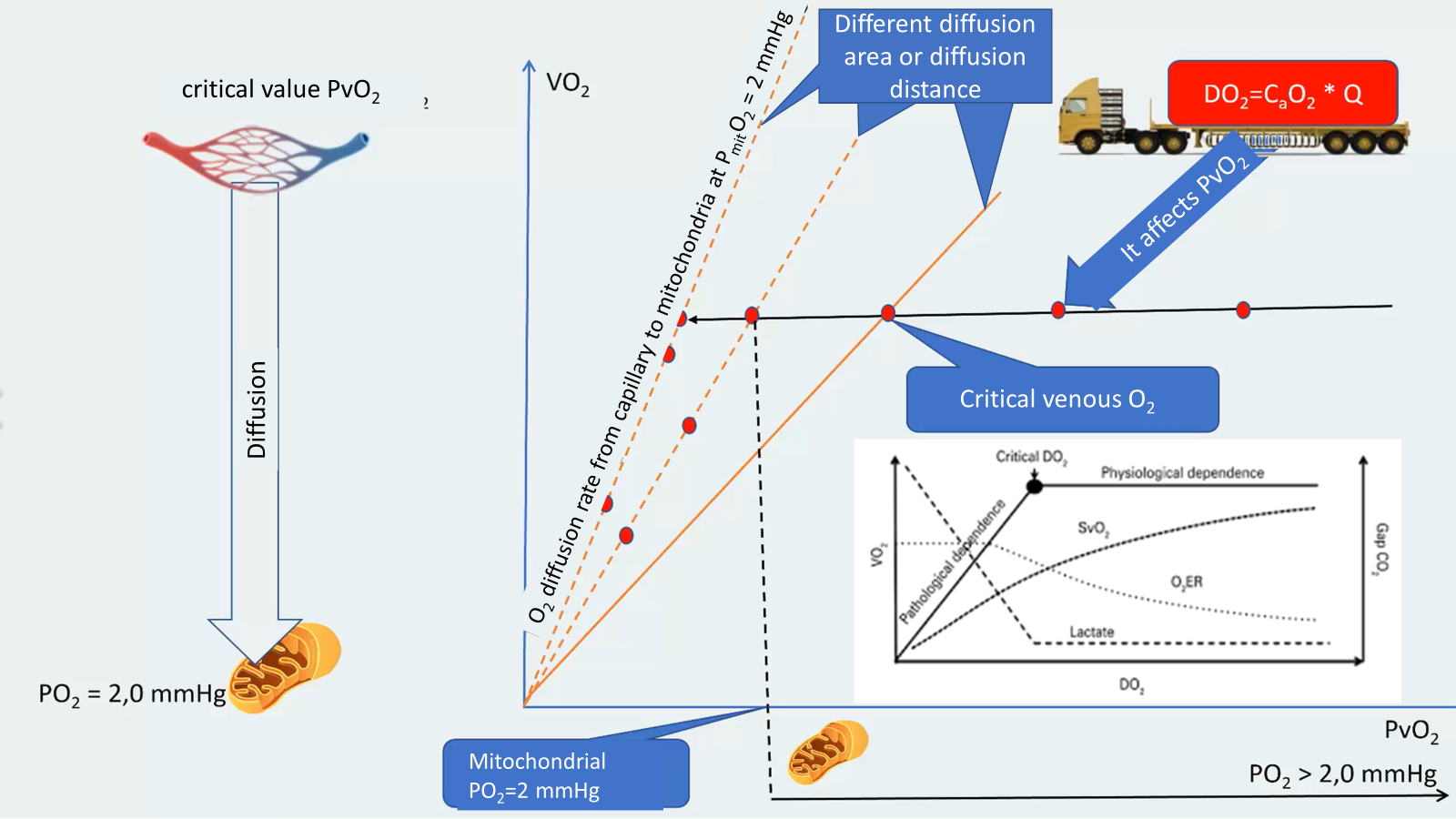
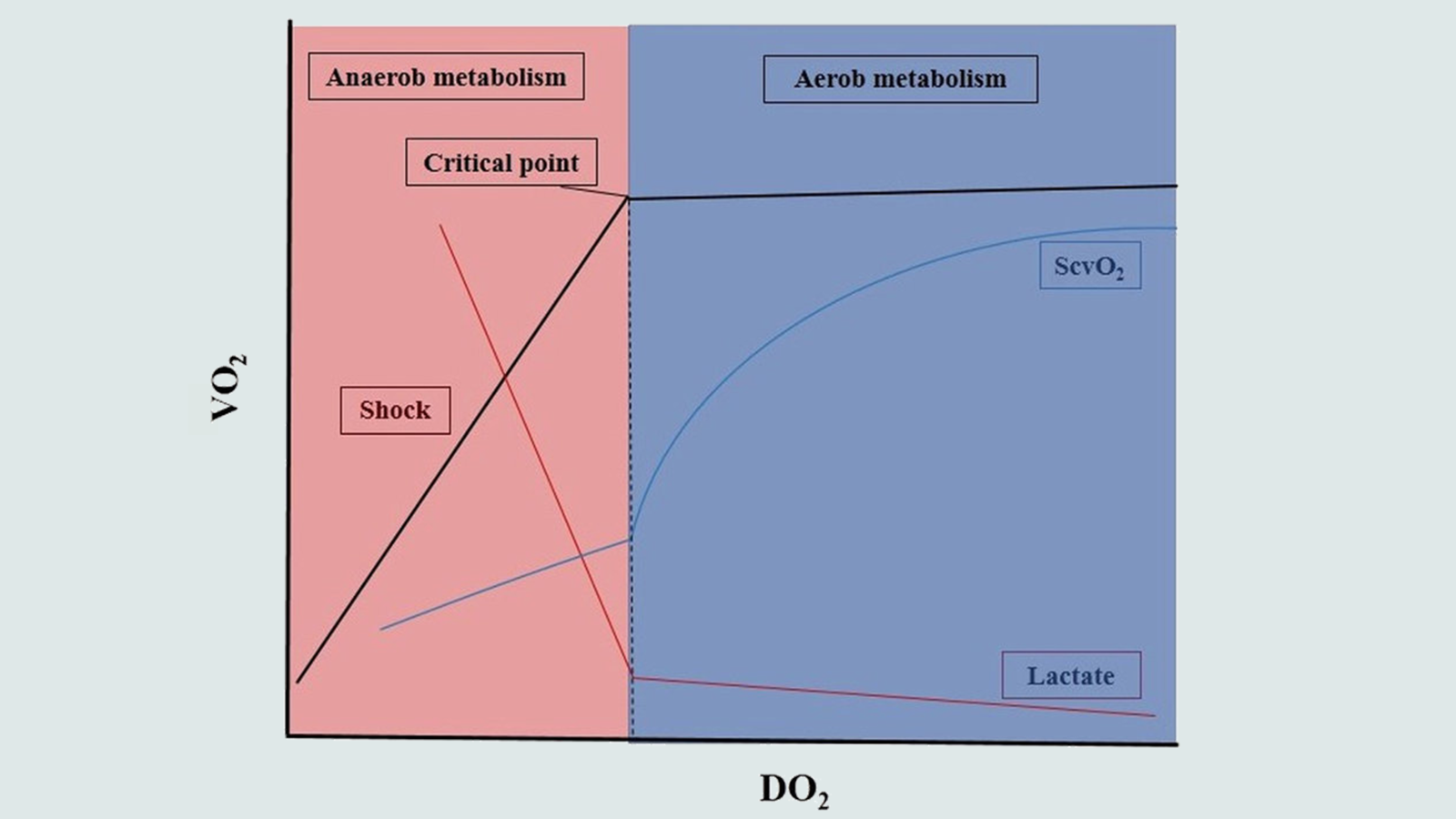
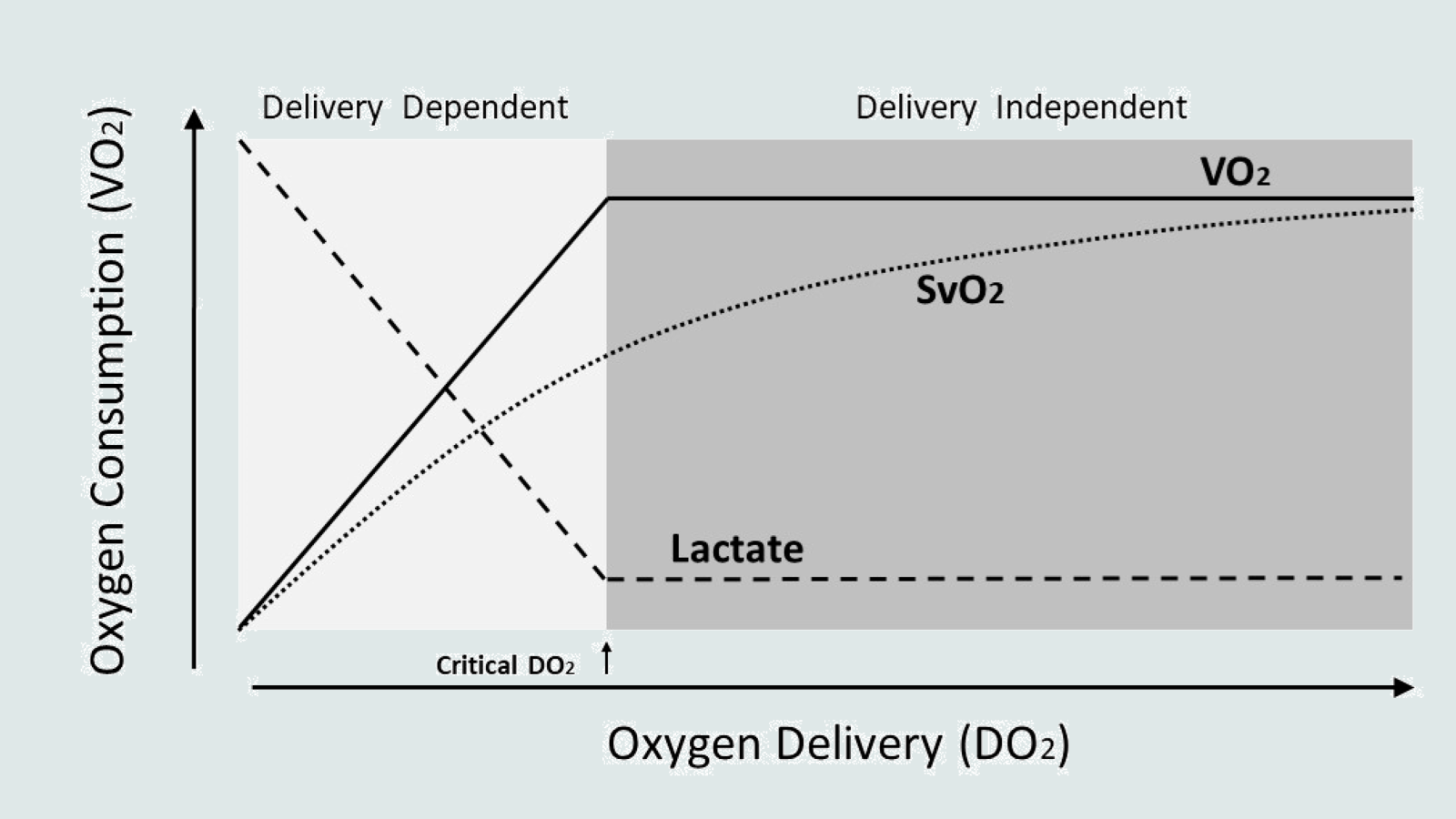
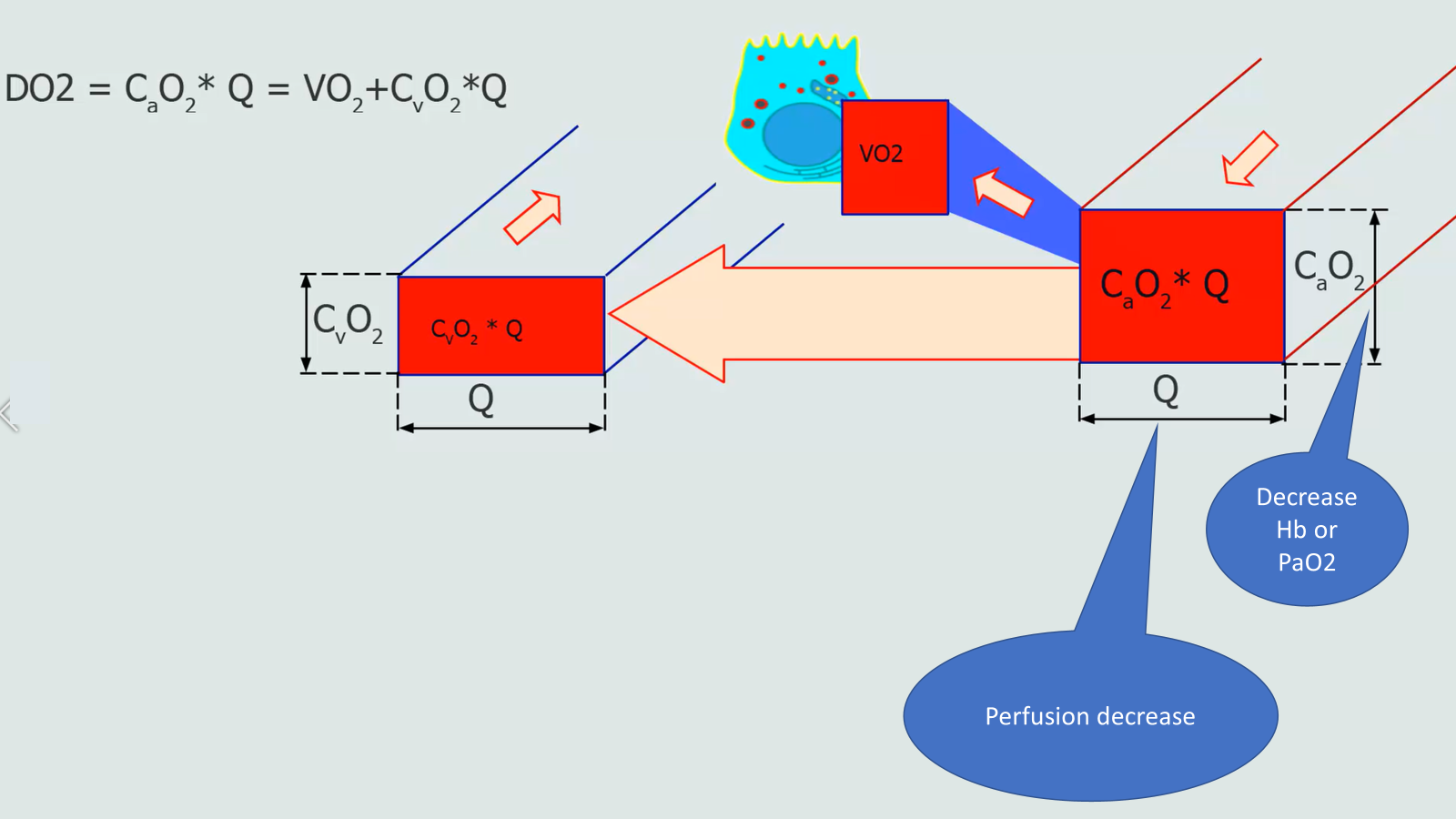
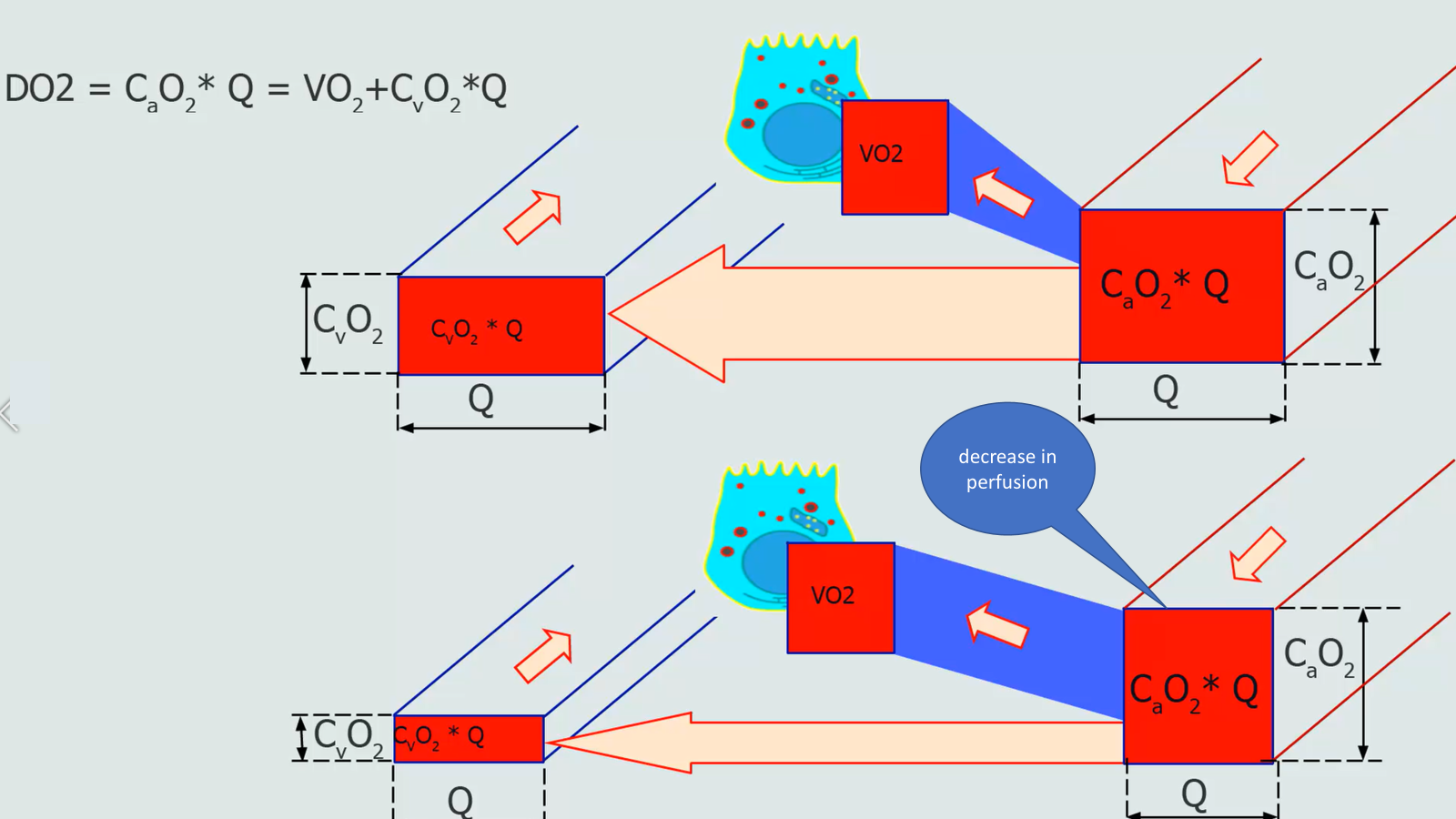
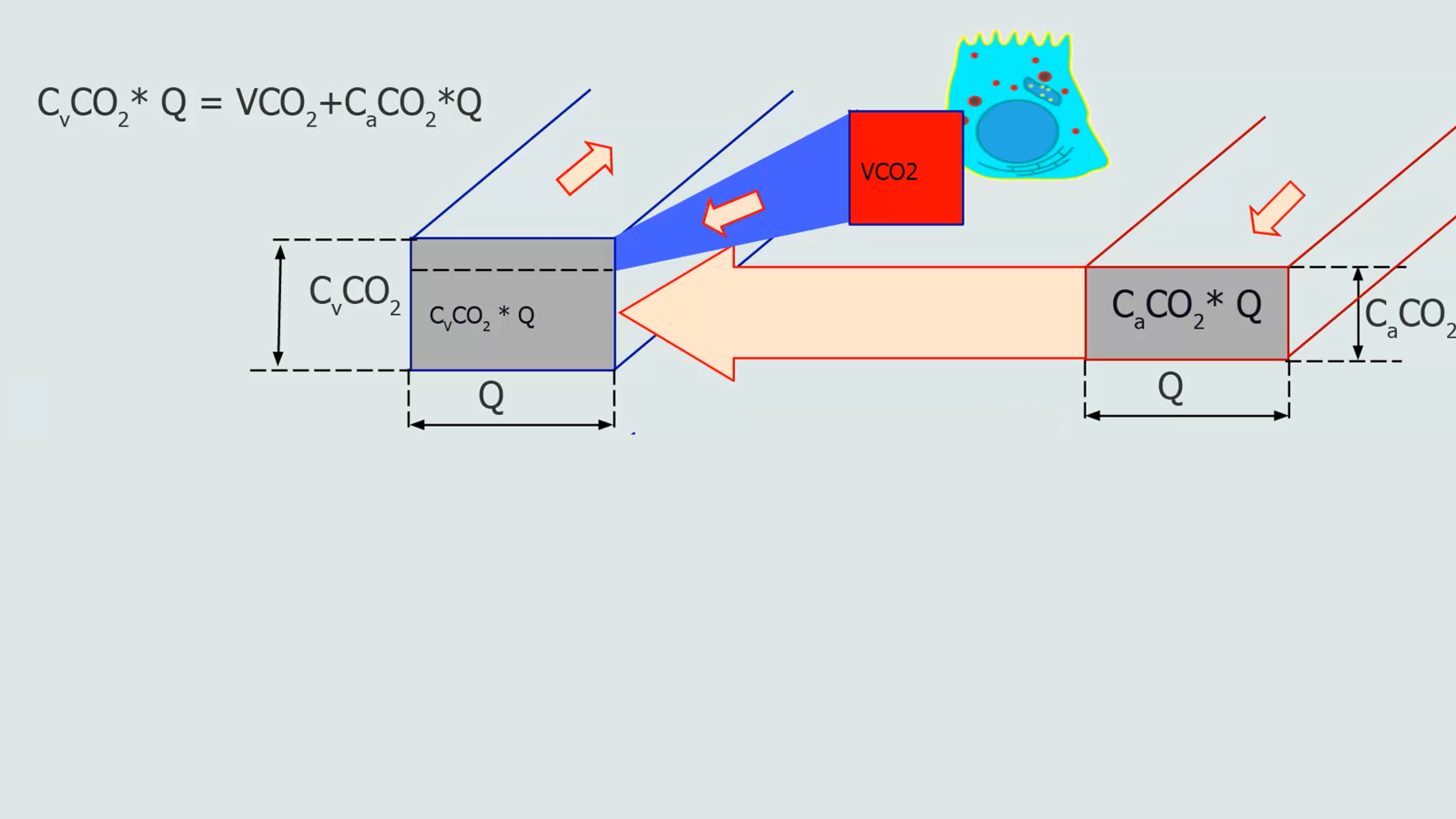

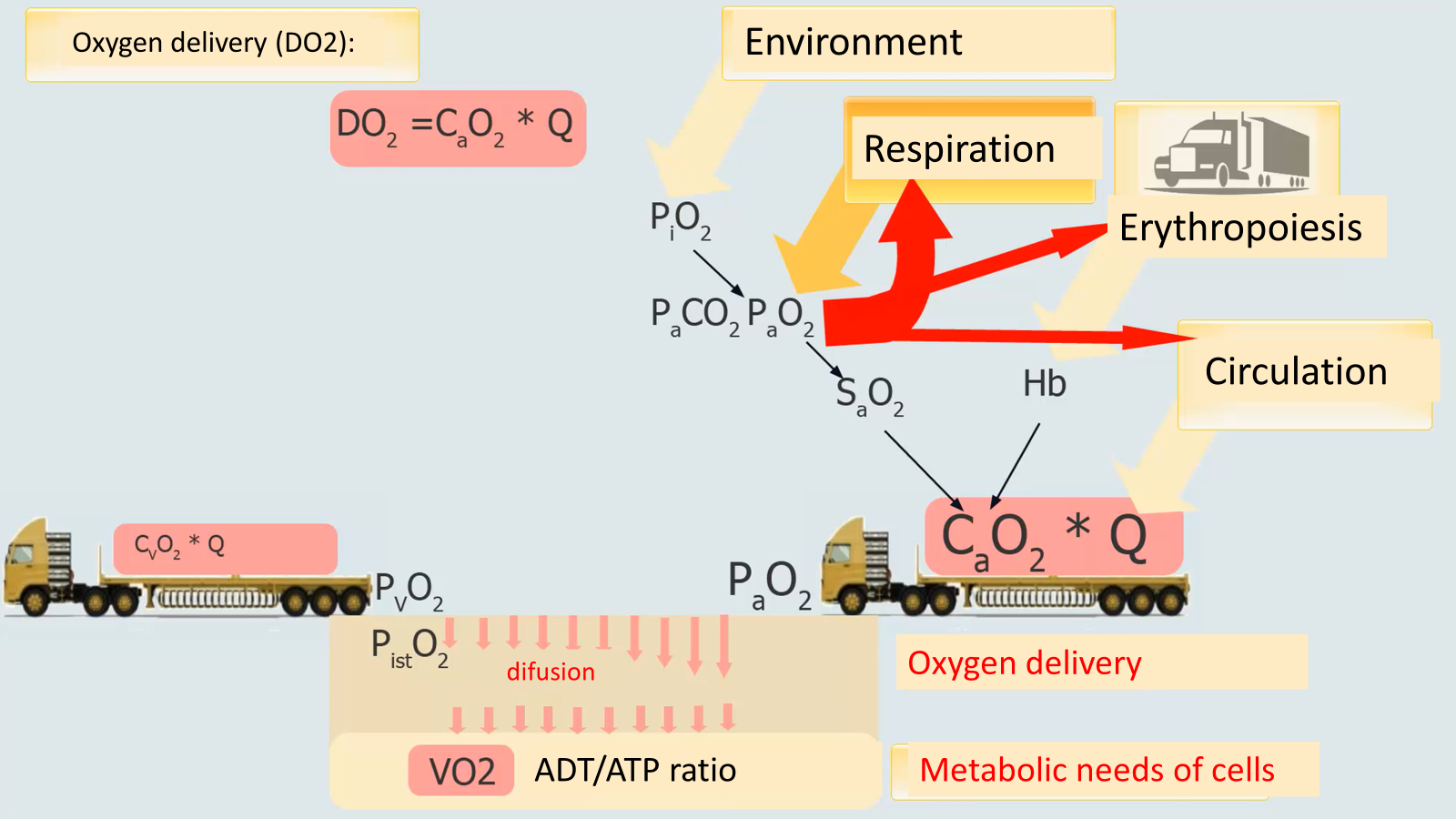
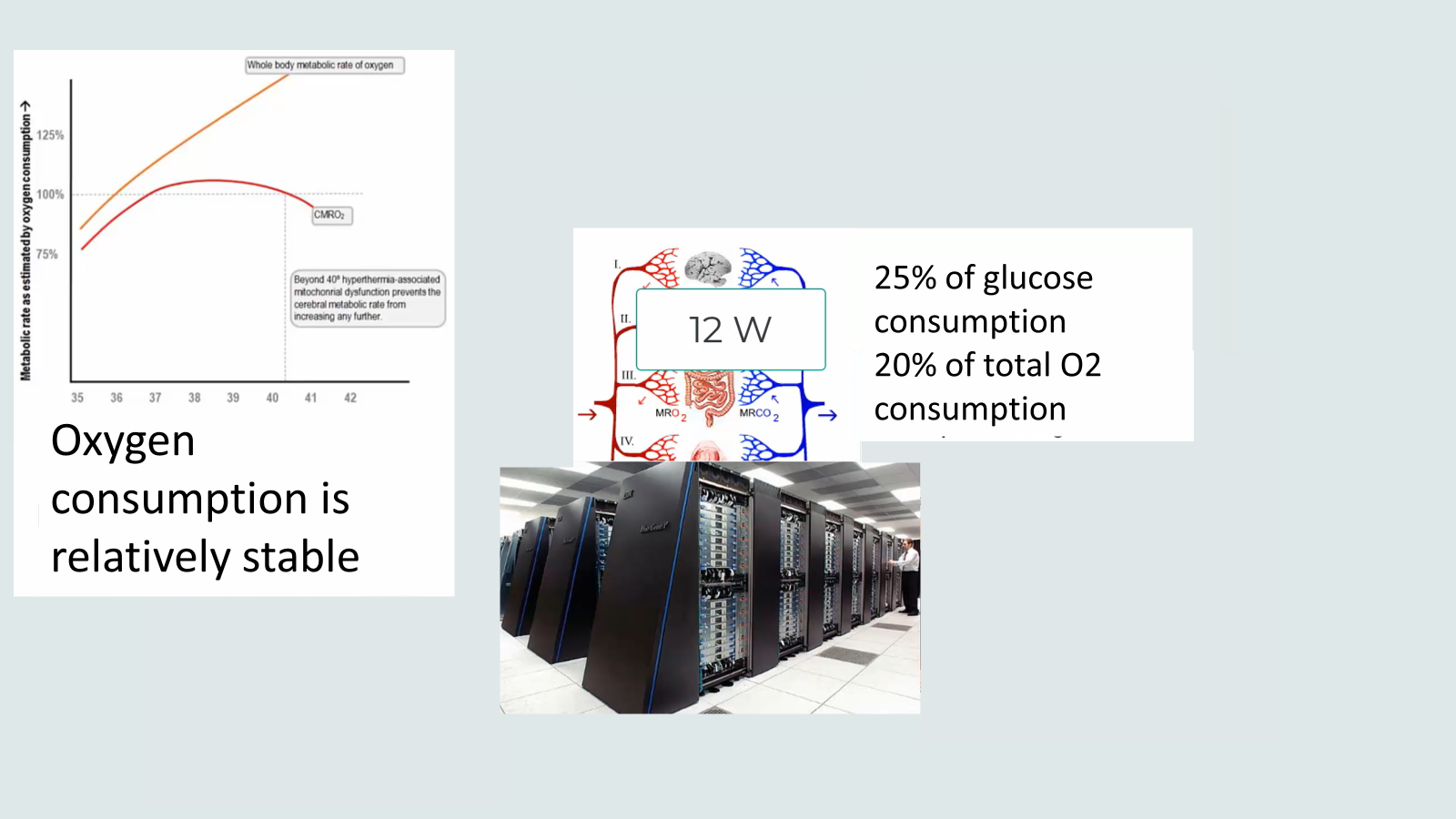
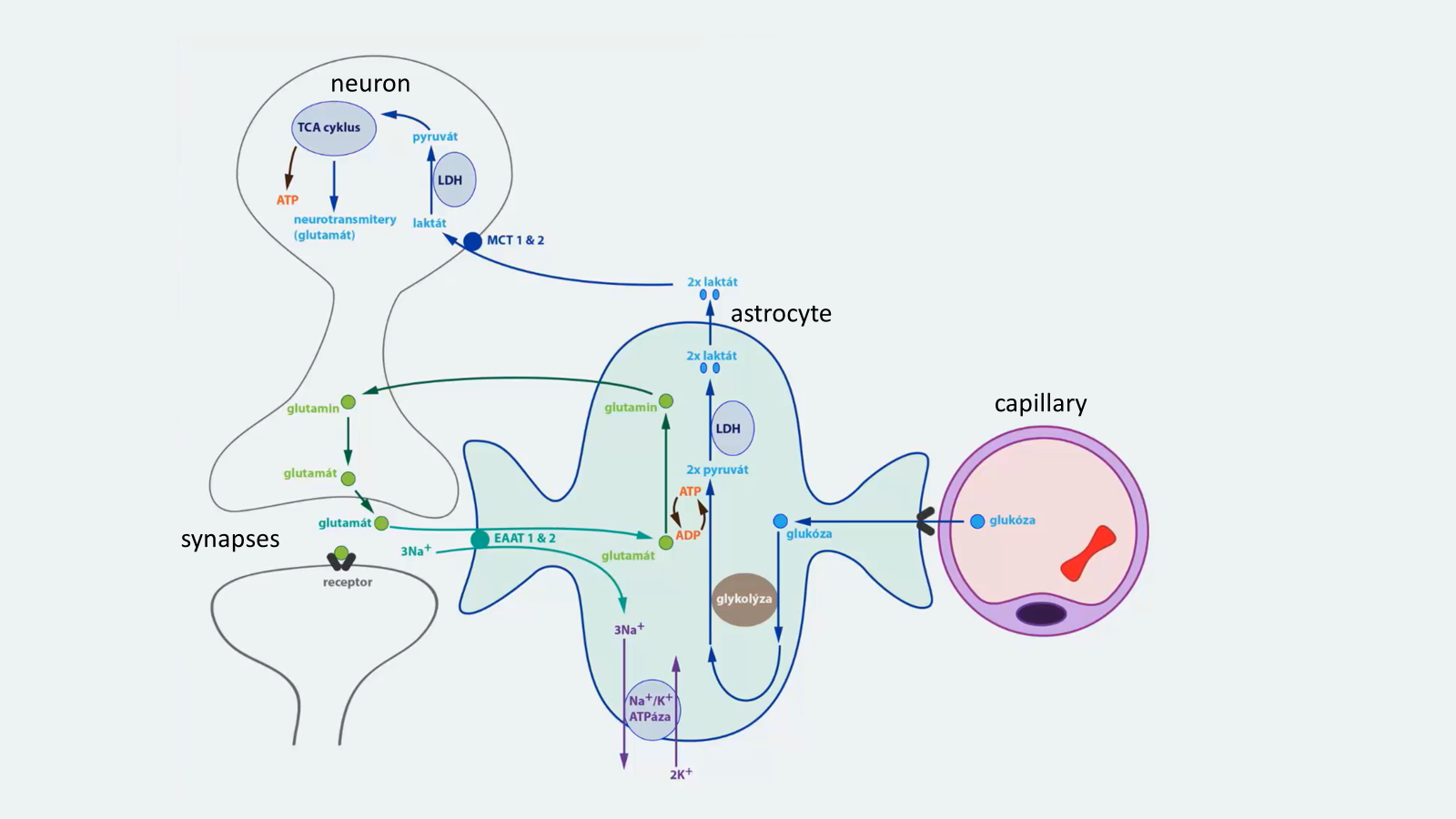
Energy generation
https://www.physiome.cz/mito_0/
https://www.physiome.cz/mito_3/